Department of Internal Medicine, 12289University of New Mexico Health Sciences Center, Albuquerque, NM, USA.
12289University of New Mexico Comprehensive Cancer Center, Albuquerque, NM, USA.
Cancer Control. 2022 Jan-Dec;29:10732748221136440. doi: 10.1177/10732748221136440.
Survival following colorectal cancer (CRC) has improved in the US since 1975, but there is limited information on stage-specific survival trends among racial and ethnic subgroups.
The purpose of this study was to estimate and compare trends in 1- and 5-year CRC cause-specific survival in the United States by both stage and race/ethnicity.
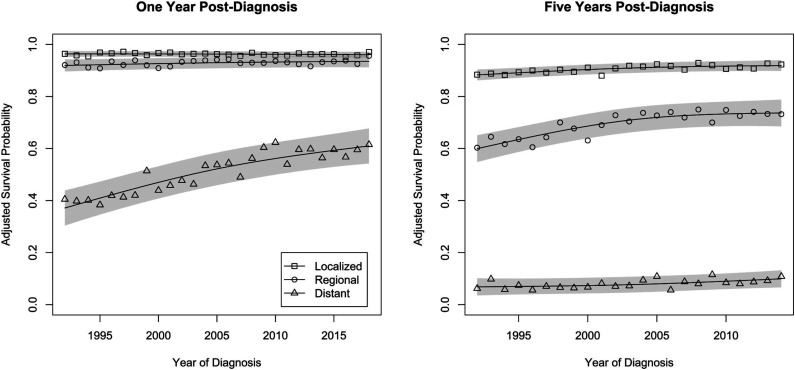
We performed a retrospective cohort study of individuals diagnosed with CRC using the 1992-2018 Surveillance, Epidemiology and End Results (SEER) database. We estimated and compared time trends in 1- and 5-year survival for CRC stage by race/ethnicity.
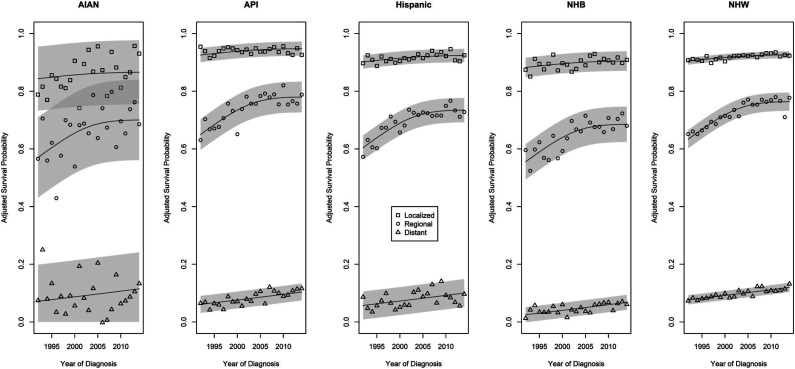
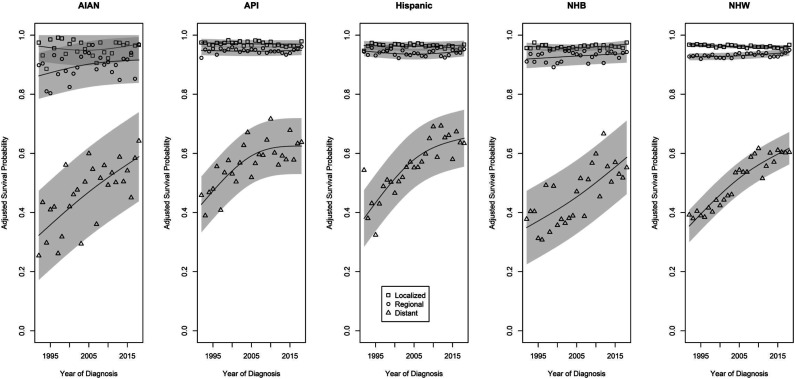
Data from 399 220 individuals diagnosed with CRC were available. There were significant differences in stage-specific 1-year survival trends by race and ethnicity. Differences were most notable for distant stage CRC: survival probabilities increased most consistently for non-Hispanic American Indian/Alaska Native (AIAN) and Black (NHB) persons, but their trend lines were lower than those of Hispanic, and non-Hispanic Asian/Pacific Islander (API) and White (NHW) persons, whose initially greater gains appear to be slowing. Although the data do not support significant racial/ethnic differences in 5-year CRC survival trends by stage, AIAN and NHB persons have the lowest average survival probabilities for multiple CRC stages, and no racial/ethnic group has 5-year survival probabilities above 20% for distant-stage CRC.
Although there has been an overall improvement in adjusted CRC-specific survival probabilities since 1992, AIAN and NHB persons continue to experience worse prognosis than those of other races/ethnicities. This highlights the importance of reinvigorating efforts to understand the causes of mortality in CRC, including those which may differ according to an individual's race or ethnicity.
自 1975 年以来,美国结直肠癌(CRC)患者的生存率有所提高,但关于不同种族和族裔亚组的特定分期生存率趋势的信息有限。
本研究旨在通过分期和种族/族裔来估计和比较美国 CRC 特定原因 1 年和 5 年生存率的趋势。
我们使用 1992 年至 2018 年的监测、流行病学和最终结果(SEER)数据库,对诊断为 CRC 的个体进行了回顾性队列研究。我们估计并比较了不同种族/族裔 CRC 分期的 1 年和 5 年生存率的时间趋势。
共有 399220 名诊断为 CRC 的个体的数据可用。不同种族和族裔的特定分期 1 年生存率趋势存在显著差异。在远处分期 CRC 中,差异最为显著:非西班牙裔美洲印第安人/阿拉斯加原住民(AIAN)和黑人(NHB)患者的生存概率增加最为一致,但他们的趋势线低于西班牙裔和非西班牙裔亚裔/太平洋岛民(API)和白人(NHW)患者,后者最初的收益似乎正在放缓。尽管数据不支持按分期的 CRC 生存趋势存在显著的种族/族裔差异,但 AIAN 和 NHB 患者在多个 CRC 分期的平均生存概率最低,没有任何种族/族裔群体的远处分期 CRC 5 年生存率超过 20%。
尽管自 1992 年以来,CRC 特异性调整后生存率总体有所提高,但 AIAN 和 NHB 患者的预后仍比其他种族/族裔差。这突显了重新努力了解 CRC 死亡率的原因的重要性,包括那些可能因个体的种族或族裔而异的原因。