Morbid Obesity Centre, Vestfold Hospital Trust, Tønsberg, Norway.
Department of Medicine, Vestfold Hospital Trust, Tønsberg, Norway.
BMC Gastroenterol. 2022 Nov 7;22(1):448. doi: 10.1186/s12876-022-02550-0.
Obesity, non-alcoholic fatty liver disease (NAFLD) and insulin resistance are three pathological conditions highly correlated, but this relationship is not fully elucidated. Hence, we aimed to assess the association of hepatic steatosis and fibrosis with different measures of insulin sensitivity in patients with severe obesity and type 2 diabetes mellitus (T2DM).
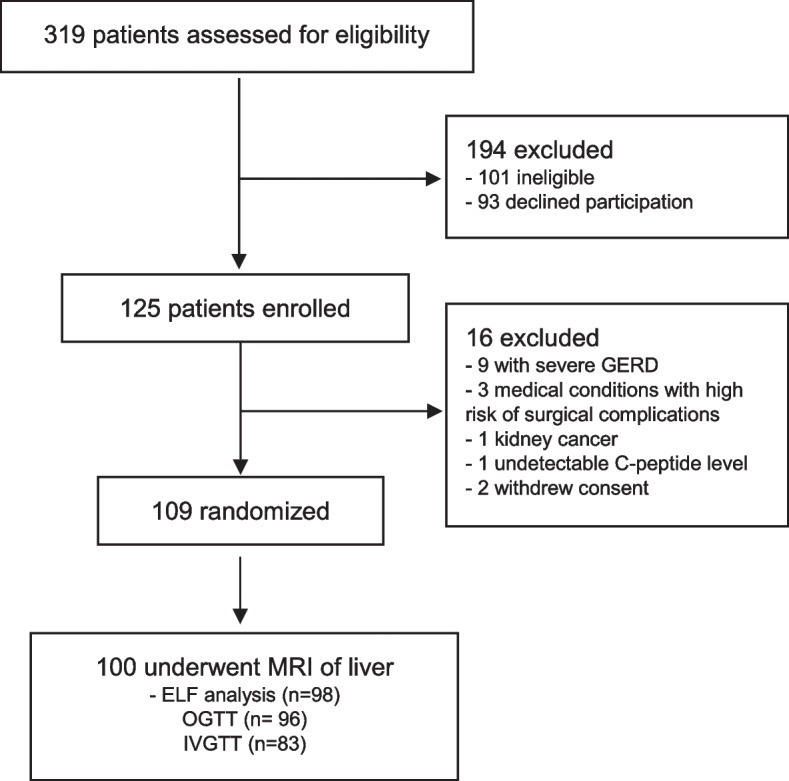
A cross-sectional study (Oseberg trial) including patients with T2DM referred for bariatric surgery at Vestfold Hospital Trust, Norway. Magnetic resonance imaging (MRI) and the enhanced liver fibrosis (ELF) test was used for estimation of liver fat fraction (LFF) and degree of fibrosis, respectively. Oral and intravenous glucose tolerance tests were applied for estimation of insulin sensitivity (HOMA2S, Matsuda ISI and MinMod SI).
A total of 100 patients (mean [SD] age 47.5 [9.7] years, 65% women, BMI 42.0 [5.3] kg/m and 98% with metabolic syndrome) were included in the analyses. The mean (SD) LFF in the total population was 19.1 (11.5), and the mean (SD) ELF score was 8.46 (0.84), a value representing moderate fibrosis. LFF was inversely associated with HOMA2S and Matsuda ISI, and both measures were significantly higher in the no or low-grade steatosis group compared with the medium-to-high grade steatosis group (mean difference [95% CI] 5.9 [2.2-9.6]%, Cohen's d = 0.75), and (0.7 [0.3-1.1], Cohen's d = 0.80, respectively). There was no association between LFF, as a categorical or continuous variable, and MinMod SI. The proportions of patients with none to mild fibrosis, moderate fibrosis and severe fibrosis were 14, 78 and 6%, respectively, and there were no significant associations between level of fibrosis and measures of insulin sensitivity.
Patients with morbid obesity and T2DM demonstrated high levels of liver fat fraction, and we showed that hepatic steatosis, but not the degree of liver fibrosis, was associated with different measures of insulin sensitivity in patients with severe obesity and T2DM. Further, our results might indicate that the LFF is primarily associated with hepatic, and not peripheral insulin sensitivity. To improve the diagnosis of NAFLD and the prediction of its progression, more studies are needed to reveal the pathological mechanistic pathways involved in NAFLD and insulin sensitivity.
ClinicalTrials.gov: NCT01778738.
肥胖、非酒精性脂肪性肝病(NAFLD)和胰岛素抵抗是三种高度相关的病理状态,但这种关系尚未完全阐明。因此,我们旨在评估严重肥胖和 2 型糖尿病(T2DM)患者肝脂肪变性和纤维化与不同胰岛素敏感性指标的相关性。
这是一项横断面研究(Oseberg 试验),纳入了在挪威 Vestfold 医院信托基金接受减重手术的 T2DM 患者。磁共振成像(MRI)和增强肝脏纤维化(ELF)试验分别用于估计肝脂肪分数(LFF)和纤维化程度。口服和静脉葡萄糖耐量试验用于估计胰岛素敏感性(HOMA2S、Matsuda ISI 和 MinMod SI)。
共有 100 名患者(平均[标准差]年龄 47.5[9.7]岁,65%为女性,BMI 42.0[5.3]kg/m2,98%患有代谢综合征)纳入了分析。总人群的平均(标准差)LFF 为 19.1(11.5),平均(标准差)ELF 评分 8.46(0.84),表示中度纤维化。LFF 与 HOMA2S 和 Matsuda ISI 呈负相关,与中重度脂肪变性组相比,无或轻度脂肪变性组的这两个指标均显著升高(平均差异[95%置信区间]5.9[2.2-9.6]%,Cohen's d=0.75),(0.7[0.3-1.1],Cohen's d=0.80)。LFF 作为分类或连续变量与 MinMod SI 之间无关联。无或轻度纤维化、中度纤维化和重度纤维化的患者比例分别为 14%、78%和 6%,纤维化程度与胰岛素敏感性指标之间无显著相关性。
患有严重肥胖和 T2DM 的患者表现出高水平的肝脂肪分数,我们表明,肝脂肪变性,但不是肝纤维化程度,与严重肥胖和 T2DM 患者的不同胰岛素敏感性指标相关。此外,我们的结果可能表明,LFF 主要与肝胰岛素敏感性相关,而与外周胰岛素敏感性无关。为了改善 NAFLD 的诊断和预测其进展,需要更多的研究来揭示涉及 NAFLD 和胰岛素敏感性的病理机制途径。
ClinicalTrials.gov:NCT01778738。