Stanford University Department of Medicine Palo Alto CA.
Stanford University Department of Biomedical Data Science Stanford CA.
J Am Heart Assoc. 2023 Feb 7;12(3):e028562. doi: 10.1161/JAHA.122.028562.
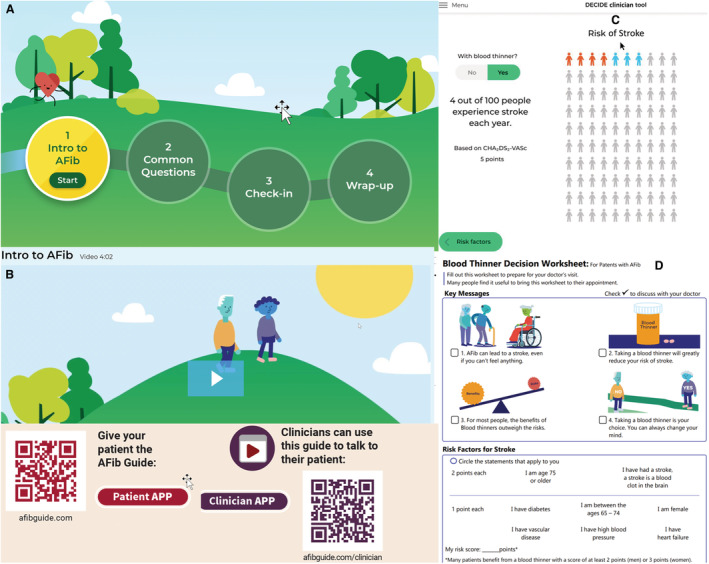
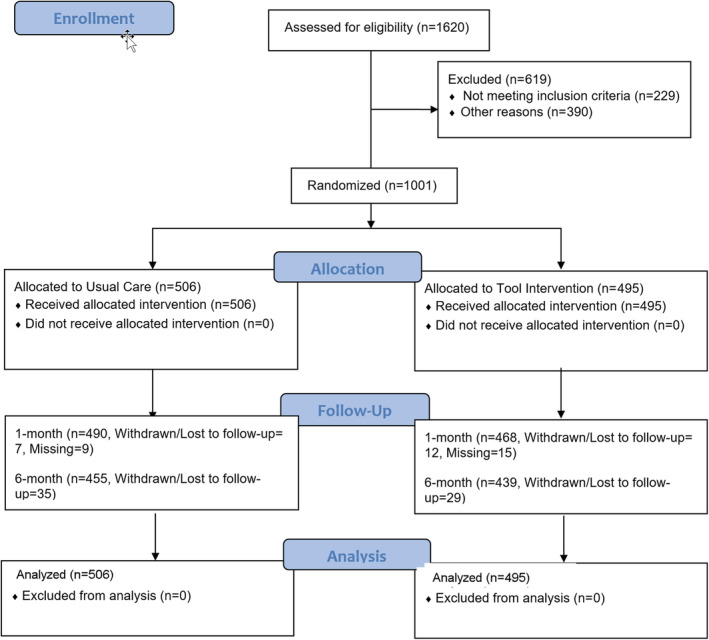
Background Oral anticoagulation reduces stroke and disability in atrial fibrillation (AF) but is underused. We evaluated the effects of a novel patient-clinician shared decision-making (SDM) tool in reducing oral anticoagulation patient's decisional conflict as compared with usual care. Methods and Results We designed and evaluated a new digital decision aid in a multicenter, randomized, comparative effectiveness trial, ENHANCE-AF (Engaging Patients to Help Achieve Increased Patient Choice and Engagement for AF Stroke Prevention). The digital AF shared decision-making toolkit was developed using patient-centered design with clear health communication principles (eg, meaningful images, limited text). Available in English and Spanish, the toolkit included the following: (1) a brief animated video; (2) interactive questions with answers; (3) a quiz to check on understanding; (4) a worksheet to be used by the patient during the encounter; and (5) an online guide for clinicians. The study population included English or Spanish speakers with nonvalvular AF and a CHADS-VASc stroke score ≥1 for men or ≥2 for women. Participants were randomized in a 1:1 ratio to either usual care or the shared decision-making toolkit. The primary end point was the validated 16-item Decision Conflict Scale at 1 month. Secondary outcomes included Decision Conflict Scale at 6 months and the 10-item Decision Regret Scale at 1 and 6 months as well as a weighted average of Mann-Whitney -statistics for both the Decision Conflict Scale and the Decision Regret Scale. A total of 1001 participants were enrolled and followed at 5 different sites in the United States between December 18, 2019, and August 17, 2022. The mean patient age was 69±10 years (40% women, 16.9% Black, 4.5% Hispanic, 3.6% Asian), and 50% of participants had CHADS-VASc scores ≥3 (men) or ≥4 (women). The primary end point at 1 month showed a clinically meaningful reduction in decisional conflict: a 7-point difference in median scores between the 2 arms (16.4 versus 9.4; Mann-Whitney -statistics=0.550; =0.007). For the secondary end point of 1-month Decision Regret Scale, the difference in median scores between arms was 5 points in the direction of less decisional regret (=0.078). The treatment effects lessened over time: at 6 months the difference in medians was 4.7 points for Decision Conflict Scale (=0.060) and 0 points for Decision Regret Scale (=0.35). Conclusions Implementation of a novel shared decision-making toolkit (afibguide.com; afibguide.com/clinician) achieved significantly lower decisional conflict compared with usual care in patients with AF. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT04096781.
口服抗凝剂可降低房颤(AF)患者的中风和残疾风险,但使用率较低。我们评估了一种新的医患共同决策(SDM)工具在降低口服抗凝患者决策冲突方面的效果,与常规护理相比。
我们在一项多中心、随机、对照效果试验 ENHANCE-AF(增强患者参与以增加 AF 中风预防的选择和参与)中设计并评估了一种新的数字决策辅助工具。数字 AF 共同决策工具包使用以患者为中心的设计和明确的健康沟通原则(例如,有意义的图像,有限的文本)开发。该工具包有英语和西班牙语两种版本,包括以下内容:(1)简短的动画视频;(2)带有答案的互动问题;(3)测验以检查理解;(4)供患者在就诊期间使用的工作表;(5)临床医生在线指南。研究人群包括讲英语或西班牙语、非瓣膜性房颤且 CHADS-VASc 中风评分男性≥1 分或女性≥2 分的患者。参与者以 1:1 的比例随机分为常规护理或共同决策工具包组。主要终点是 1 个月时经过验证的 16 项决策冲突量表。次要结局包括 6 个月时决策冲突量表和 1 个月和 6 个月时的 10 项决策后悔量表,以及决策冲突量表和决策后悔量表的曼-惠特尼 -统计加权平均值。共有 1001 名参与者在 2019 年 12 月 18 日至 2022 年 8 月 17 日在美国的 5 个不同地点入组并随访。患者平均年龄为 69±10 岁(40%为女性,16.9%为黑人,4.5%为西班牙裔,3.6%为亚洲人),50%的参与者 CHADS-VASc 评分≥3(男性)或≥4(女性)。1 个月时的主要终点显示决策冲突有明显的临床改善:两组中位数评分相差 7 分(16.4 与 9.4;曼-惠特尼 -统计=0.550;=0.007)。次要终点 1 个月决策后悔量表的中位数评分差值为 5 分,表明后悔程度较低(=0.078)。治疗效果随时间减弱:6 个月时决策冲突量表的中位数差值为 4.7 分(=0.060),决策后悔量表的中位数差值为 0 分(=0.35)。
与常规护理相比,新型共同决策工具包(afibguide.com;afibguide.com/clinician)的实施可显著降低房颤患者的决策冲突。