Norwegian National Centre for Ageing and Health, Vestfold Hospital Trust, PO Box 2136, Tønsberg, 3103, Norway.
Faculty of Health Sciences and Social Care, Molde University College, Molde, Norway.
BMC Public Health. 2022 Nov 8;22(1):2046. doi: 10.1186/s12889-022-14433-w.
Several modifiable lifestyle risk factors for dementia have been identified, but it is unclear how much the Norwegian public knows about the relationship between lifestyle and brain health. Therefore, this study aimed to investigate knowledge about modifiable dementia risk and protective factors and beliefs and attitudes towards dementia and dementia risk reduction in a randomly selected subsample of the Norwegian population.
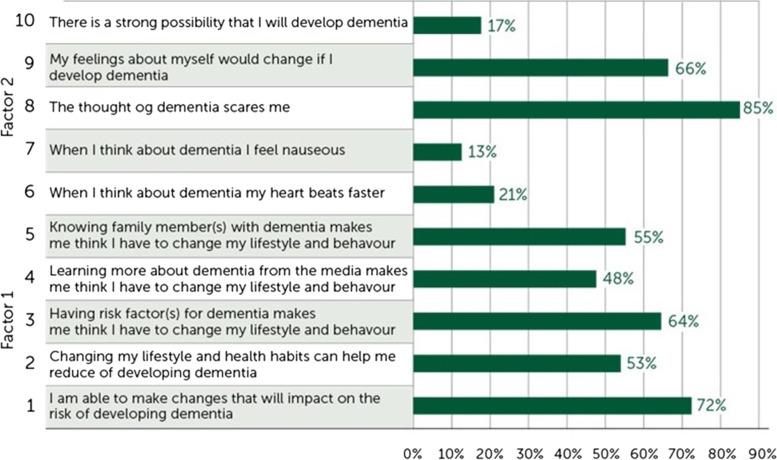
The total sample (n = 1435) included individuals aged 40-70 years from four counties (Oslo, Innlandet, Nordland and Trøndelag) in Norway. Two online questionnaires were used to measure (1) awareness about dementia risk reduction and (2) an individual`s motivation to change behaviour for dementia risk reduction (MOCHAD-10).
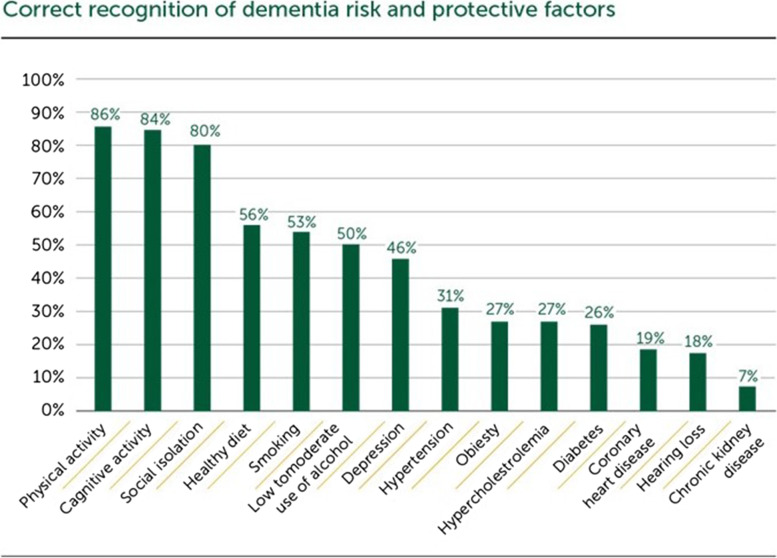
Of the participants, 70% were aware of the potential of dementia risk reduction in general. Physical inactivity (86%), cognitive inactivity (84%) and social isolation (80%) were the most frequently recognised dementia risk factors. On the other hand, diabetes (26%), coronary heart disease (19%), hearing loss (18%) and chronic kidney disease (7%) were less often recognised as dementia risk factors. Comparing men and women, the only significant difference was that women were more likely to report parents with dementia as a risk factor compared to men. Gender, age and educational differences were seen in beliefs and attitudes towards dementia prevention:women reported more negative feelings and attitudes towards dementia than men;those aged 40-49 years - more likely than older age groups - reported that 'knowing family members with dementia' or 'having risk factors' made them believe they had to change their lifestyle and behaviour.
The results indicate that 70% of the Norwegian public are aware of the potential for dementia risk reduction in general. However, there are major gaps in existing knowledge, particularly for cardiovascular risk factors such as hypertension, coronary heart disease, hypercholesterolemia and metabolic factors (diabetes, obesity). These findings underline the importance of further informing the Norwegian public about lifestyle-related risk and protective factors of dementia. Differences in beliefs and attitudes towards dementia risk prevention by age, gender and education require tailored public risk reduction interventions.
已经确定了几种可改变的痴呆症生活方式风险因素,但尚不清楚挪威公众对生活方式与大脑健康之间的关系了解多少。因此,本研究旨在调查随机选择的挪威人群中的一个亚样本对可改变的痴呆症风险和保护因素的认识,以及对痴呆症和痴呆症风险降低的信念和态度。
总样本(n=1435)包括来自挪威四个县(奥斯陆、因内尔兰、诺尔兰和特隆德拉格)的 40-70 岁人群。使用两个在线问卷来衡量(1)对痴呆症风险降低的认识,以及(2)个人对降低痴呆症风险改变行为的动机(MOCHAD-10)。
在参与者中,有 70%的人普遍意识到痴呆症风险降低的可能性。身体不活动(86%)、认知不活动(84%)和社会孤立(80%)是最常被认为的痴呆症风险因素。另一方面,糖尿病(26%)、冠心病(19%)、听力损失(18%)和慢性肾脏病(7%)则较少被认为是痴呆症风险因素。将男性和女性进行比较,唯一的显著差异是女性比男性更有可能将父母患有痴呆症报告为风险因素。在对痴呆症预防的信念和态度方面存在性别、年龄和教育差异:女性比男性报告更多的对痴呆症的负面感受和态度;40-49 岁的人比年龄较大的人群更有可能报告说“认识有痴呆症的家庭成员”或“有风险因素”,这使他们认为必须改变生活方式和行为。
结果表明,70%的挪威公众普遍意识到痴呆症风险降低的可能性。然而,现有的知识存在重大差距,特别是对于心血管风险因素,如高血压、冠心病、高胆固醇血症和代谢因素(糖尿病、肥胖症)。这些发现强调了进一步向挪威公众宣传与生活方式相关的痴呆症风险和保护因素的重要性。年龄、性别和教育程度对痴呆症风险预防的信念和态度的差异需要有针对性的公众风险降低干预措施。