Howard-Jones Annaleise R, Sparks Rebecca, Pham David, Halliday Catriona, Beardsley Justin, Chen Sharon C-A
Centre for Infectious Diseases & Microbiology Laboratory Services, New South Wales Health Pathology-Institute of Clinical Pathology & Medical Research, Westmead Hospital, Westmead, NSW 2145, Australia.
Faculty of Medicine and Health, University of Sydney, Camperdown, NSW 2145, Australia.
J Fungi (Basel). 2022 Oct 31;8(11):1156. doi: 10.3390/jof8111156.
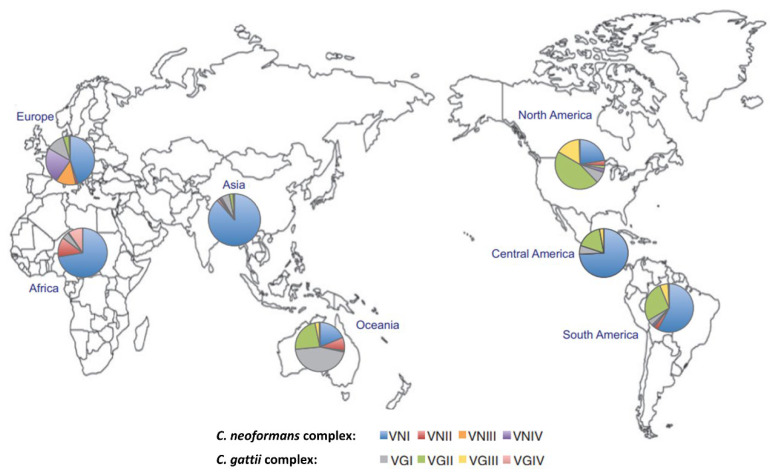
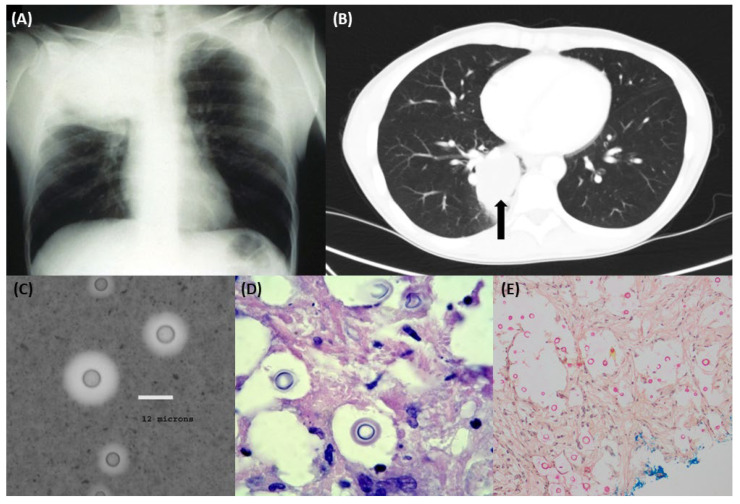
Pulmonary cryptococcosis describes an invasive lung mycosis caused by or complex. It is often a high-consequence disease in both immunocompromised and immunocompetent populations, and may be misdiagnosed as pulmonary malignancy, leading to a delay in therapy. Epidemiology follows that of cryptococcal meningoencephalitis, with infection more common in certain geographic regions. Diagnostic tools include histopathology, microscopy and culture, and the detection of cryptococcal polysaccharide antigen or -derived nucleic acids. All patients with lung cryptococcosis should have a lumbar puncture and cerebral imaging to exclude central nervous system disease. Radiology is key, both as an adjunct to laboratory testing and as the initial means of detection in asymptomatic patients or those with non-specific symptoms. Pulmonary cryptococcomas (single or multiple) may also be associated with disseminated disease and/or cryptococcal meningitis, requiring prolonged treatment regimens. Optimal management for severe disease requires extended induction (amphotericin B and flucytosine) and consolidation therapy (fluconazole) with close clinical monitoring. Susceptibility testing is of value for epidemiology and in regions where relatively high minimum inhibitory concentrations to azoles (particularly fluconazole) have been noted. Novel diagnostic tools and therapeutic agents promise to improve the detection and treatment of cryptococcosis, particularly in low-income settings where the disease burden is high.
肺隐球菌病是指由新型隐球菌或格特隐球菌复合体引起的一种侵袭性肺部真菌病。在免疫功能低下和免疫功能正常人群中,它往往是一种后果严重的疾病,可能被误诊为肺部恶性肿瘤,从而导致治疗延误。其流行病学情况与隐球菌性脑膜脑炎相似,在某些地理区域,新型隐球菌感染更为常见。诊断工具包括组织病理学、显微镜检查和培养,以及检测隐球菌多糖抗原或其衍生的核酸。所有肺隐球菌病患者均应进行腰椎穿刺和脑部影像学检查,以排除中枢神经系统疾病。放射学检查至关重要,它既是实验室检测的辅助手段,也是无症状患者或有非特异性症状患者的初始检测方法。肺隐球菌瘤(单发或多发)也可能与播散性疾病和/或隐球菌性脑膜炎相关,需要延长治疗方案。重症疾病的最佳管理需要延长诱导期(两性霉素B和氟胞嘧啶)和巩固期治疗(氟康唑),并进行密切的临床监测。药敏试验对于流行病学研究以及在已注意到对唑类(尤其是氟康唑)的最低抑菌浓度相对较高的地区具有重要价值。新型诊断工具和治疗药物有望改善隐球菌病的检测和治疗,特别是在疾病负担较高的低收入环境中。