Centre for Evidence Based Healthcare, Division of Epidemiology and Public Health, Clinical Sciences Building Phase 2, University of Nottingham, Nottingham, UK.
Global Health Division, RTI International, Washington DC, USA.
Cochrane Database Syst Rev. 2022 Nov 11;11(11):CD008923. doi: 10.1002/14651858.CD008923.pub3.
Larval source management (LSM) may help reduce Plasmodium parasite transmission in malaria-endemic areas. LSM approaches include habitat modification (permanently or temporarily reducing mosquito breeding aquatic habitats); habitat manipulation (temporary or recurrent change to environment); or use of chemical (e.g. larviciding) or biological agents (e.g. natural predators) to breeding sites. We examined the effectiveness of habitat modification or manipulation (or both), with and without larviciding. This is an update of a review published in 2013.
We used standard, extensive Cochrane search methods. The latest search was from January 2012 to 30 November 2021.
Randomized controlled trials (RCT) and non-randomized intervention studies comparing mosquito aquatic habitat modification or manipulation (or both) to no treatment or another active intervention. We also included uncontrolled before-after (BA) studies, but only described and summarized the interventions from studies with these designs. Primary outcomes were clinical malaria incidence, malaria parasite prevalence, and malaria parasitaemia incidence.
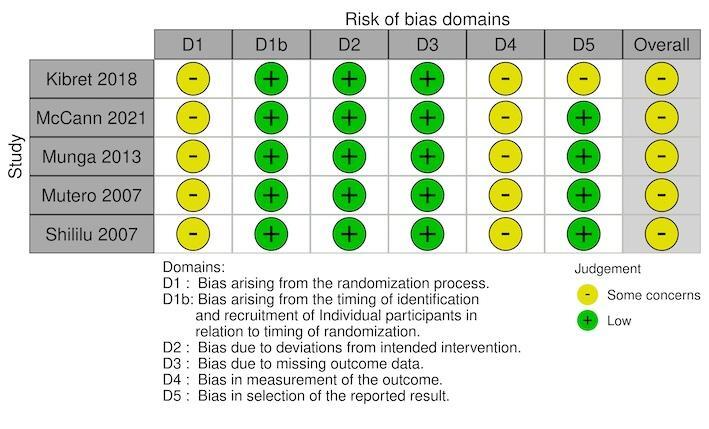
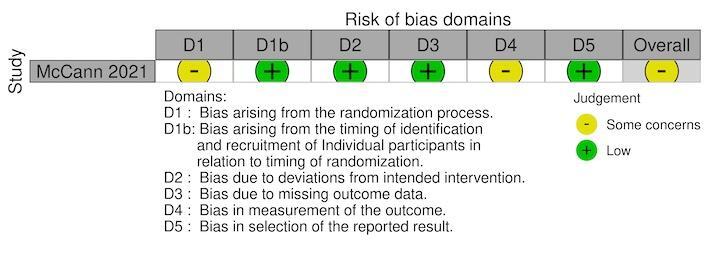
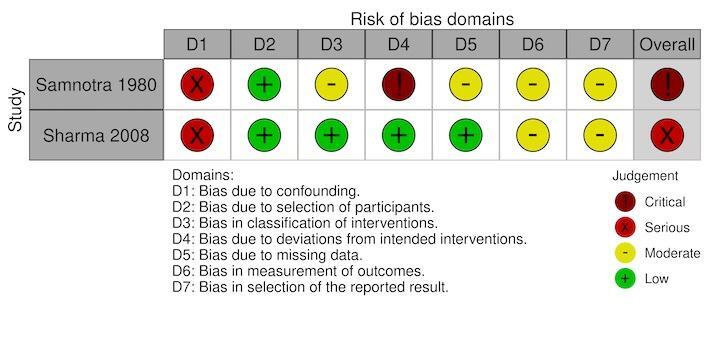
We used standard Cochrane methods. We assessed risk of bias using the Cochrane RoB 2 tool for RCTs and the ROBINS-I tool for non-randomized intervention studies. We used a narrative synthesis approach to systematically describe and summarize all the interventions included within the review, categorized by the type of intervention (habitat modification, habitat manipulation, combination of habitat modification and manipulation). Our primary outcomes were 1. clinical malaria incidence; 2. malaria parasite prevalence; and 3. malaria parasitaemia incidence. Our secondary outcomes were 1. incidence of severe malaria; 2. anaemia prevalence; 3. mean haemoglobin levels; 4. mortality rate due to malaria; 5. hospital admissions for malaria; 6. density of immature mosquitoes; 7. density of adult mosquitoes; 8. sporozoite rate; 9. entomological inoculation rate; and 10.
We used the GRADE approach to assess the certainty of the evidence for each type of intervention.
Sixteen studies met the inclusion criteria. Six used an RCT design, six used a controlled before-after (CBA) study design, three used a non-randomized controlled design, and one used an uncontrolled BA study design. Eleven studies were conducted in Africa and five in Asia. Five studies reported epidemiological outcomes and 15 studies reported entomological outcomes. None of the included studies reported on the environmental impacts associated with the intervention. For risk of bias, all trials had some concerns and other designs ranging from moderate to critical. Ten studies assessed habitat manipulation (temporary change to the environment). This included water management (spillways across streams; floodgates; intermittent flooding; different drawdown rates of water; different flooding and draining regimens), shading management (shading of drainage channels with different plants), other/combined management approaches (minimal tillage; disturbance of aquatic habitats with grass clearing and water replenishment), which showed mixed results for entomological outcomes. Spillways across streams, faster drawdown rates of water, shading drainage canals with Napier grass, and using minimal tillage may reduce the density of immature mosquitoes (range of effects from 95% reduction to 1.7 times increase; low-certainty evidence), and spillways across streams may reduce densities of adult mosquitoes compared to no intervention (low-certainty evidence). However, the effect of habitat manipulation on malaria parasite prevalence and clinical malaria incidence is uncertain (very low-certainty evidence). Two studies assessed habitat manipulation with larviciding. This included reducing or removal of habitat sites; and drain cleaning, grass cutting, and minor repairs. It is uncertain whether drain cleaning, grass cutting, and minor repairs reduces malaria parasite prevalence compared to no intervention (odds ratio 0.59, 95% confidence interval (CI) 0.42 to 0.83; very low-certainty evidence). Two studies assessed combination of habitat manipulation and permanent change (habitat modification). This included drainage canals, filling, and planting of papyrus and other reeds for shading near dams; and drainage of canals, removal of debris, land levelling, and filling ditches. Studies did not report on epidemiological outcomes, but entomological outcomes suggest that such activities may reduce the density of adult mosquitoes compared to no intervention (relative risk reduction 0.49, 95% CI 0.47 to 0.50; low-certainty evidence), and preventing water stagnating using drainage of canals, removal of debris, land levelling, and filling ditches may reduce the density of immature mosquitoes compared to no intervention (ranged from 10% to 55% reductions; low-certainty evidence). Three studies assessed combining manipulation and modification with larviciding. This included filling or drainage of water bodies; filling, draining, or elimination of rain pools and puddles at water supply points and stream bed pools; and shoreline work, improvement and maintenance to drainage, clearing vegetation and undergrowth, and filling pools. There were mixed effect sizes for the reduction of entomological outcomes (moderate-certainty evidence). However, filling or draining water bodies probably makes little or no difference to malaria parasite prevalence, haemoglobin levels, or entomological inoculation rate when delivered with larviciding compared to no intervention (moderate-certainty evidence).
AUTHORS' CONCLUSIONS: Habitat modification and manipulation interventions for preventing malaria has some indication of benefit in both epidemiological and entomological outcomes. While the data are quite mixed and further studies could help improve the knowledge base, these varied approaches may be useful in some circumstances.
幼虫源管理(LSM)可能有助于减少疟疾流行地区疟原虫的传播。LSM 方法包括:改变栖息地(永久性或暂时减少蚊虫滋生的水生栖息地);改变栖息地(环境的临时或反复变化);或使用化学(例如,杀幼虫剂)或生物制剂(例如,天然捕食者)处理滋生地。我们检查了栖息地改变或操纵(或两者兼有),并辅以杀幼虫剂的效果。这是 2013 年发表的一篇综述的更新。
我们使用了标准的、广泛的 Cochrane 检索方法。最新检索时间为 2012 年 1 月至 2021 年 11 月 30 日。
随机对照试验(RCT)和非随机干预研究比较了蚊虫水生栖息地改变或操纵(或两者兼有)与不治疗或另一种主动干预。我们还包括了未经控制的前后(BA)研究,但仅描述和总结了具有这些设计的研究中的干预措施。主要结局是临床疟疾发病率、疟疾寄生虫患病率和疟疾寄生虫血症发病率。
我们使用了标准的 Cochrane 方法。我们使用 Cochrane RoB 2 工具评估 RCT 的偏倚风险,使用 ROBINS-I 工具评估非随机干预研究的偏倚风险。我们使用叙述性综合方法系统地描述和总结了综述中包含的所有干预措施,按干预类型(栖息地改变、栖息地操纵、栖息地改变和操纵的组合)进行分类。我们的主要结局是:1. 临床疟疾发病率;2. 疟疾寄生虫患病率;3. 疟疾寄生虫血症发病率。我们的次要结局是:1. 严重疟疾发病率;2. 贫血患病率;3. 平均血红蛋白水平;4. 疟疾死亡率;5. 疟疾住院率;6. 未成熟蚊子密度;7. 成年蚊子密度;8. 孢子率;9. 昆虫接种率;10.
我们使用 GRADE 方法评估了每种干预措施的证据确定性。
有 16 项研究符合纳入标准。其中 6 项采用 RCT 设计,6 项采用对照前后(CBA)研究设计,3 项采用非随机对照设计,1 项采用未对照的 BA 研究设计。11 项研究在非洲进行,5 项在亚洲进行。5 项研究报告了流行病学结局,15 项研究报告了昆虫学结局。没有一项纳入的研究报告与干预相关的环境影响。关于偏倚风险,所有试验都存在一些问题,其他设计从中度到关键不等。10 项研究评估了栖息地操纵(环境的临时变化)。这包括水管理(溪流上的溢洪道;水闸;间歇性洪水;不同的水位下降率;不同的洪水和排水方案)、遮蔽管理(排水渠用不同的植物遮蔽)、其他/综合管理方法(最小耕作;用除草和补水扰乱水生栖息地),这些方法对昆虫学结果的影响各不相同。溪流上的溢洪道、更快的水位下降率、用 Napier 草遮蔽排水渠,以及使用最小耕作可能会降低未成熟蚊子的密度(效果范围从减少 95%到增加 1.7 倍;低确定性证据),并且溪流上的溢洪道可能会降低与无干预相比的成年蚊子的密度(低确定性证据)。然而,栖息地操纵对疟疾寄生虫患病率和临床疟疾发病率的影响尚不确定(极低确定性证据)。有 2 项研究评估了栖息地操纵与杀幼虫剂联合使用。这包括减少或清除栖息地;以及清理排水渠、割草和进行小修小补。与无干预相比,清理排水渠、割草和进行小修小补是否能降低疟疾寄生虫患病率尚不确定(比值比 0.59,95%置信区间(CI)0.42 至 0.83;低确定性证据)。有 2 项研究评估了栖息地改变和永久性改变(栖息地修饰)的组合。这包括在大坝附近的排水渠中种植纸莎草和其他芦苇以遮蔽和阴影;以及排水渠、清除杂物、土地平整和填沟。这些研究没有报告流行病学结果,但昆虫学结果表明,与无干预相比,这种活动可能会降低成年蚊子的密度(相对风险降低 0.49,95%CI 0.47 至 0.50;低确定性证据),并且通过排水渠、清除杂物、土地平整和填沟来防止水停滞不前可能会降低与无干预相比的未成熟蚊子的密度(降低 10%至 55%;低确定性证据)。有 3 项研究评估了将操纵和修饰与杀幼虫剂结合使用。这包括水体的填充或排空;填充、排空或消除供水点和河床水池的雨水池和水坑;以及岸线工作、改善和维护排水、清除植被和灌木丛以及填充水池。减少昆虫学结果的效果大小各不相同(中等确定性证据)。然而,与无干预相比,在有杀幼虫剂的情况下,填充或排空水体可能对疟疾寄生虫患病率、血红蛋白水平或昆虫接种率几乎没有影响(中等确定性证据)。
预防疟疾的栖息地改变和操纵干预措施在流行病学和昆虫学结果方面都有一定的益处。虽然数据相当混杂,进一步的研究可能有助于增加知识基础,但这些不同的方法在某些情况下可能有用。