Clinical College of Chinese Medicine, Gansu University of Chinese Medicine, Lanzhou, Gansu Province, China.
Department of Orthopedics, The Affiliated hospital of Gansu University of Chinese Medicine, Lanzhou, Gansu Province, China.
Medicine (Baltimore). 2022 Nov 11;101(45):e31562. doi: 10.1097/MD.0000000000031562.
Gout in the spine and adnexa is rare in clinical practice and can also be easily misdiagnosed, we reported a patient with nerve root compression due to lumbar gout stones in the lumbar spinal canal.
A 51-year-old male was admitted to the hospital with lumbar pain with numbness in the left lower limb for more than 6 months. The physical examination showed that tenderness and percussion pain were present at L4-S1 spinous process. Straight leg raise test: 50° on the left side were positive. Laboratory tests showed that the sUA was 669 μmol/L, MRI of the lumbar spine showed that cystic T1WI low signal and T2WI mixed high signal shadows were seen in the spinal canal at the level of L4-L5.
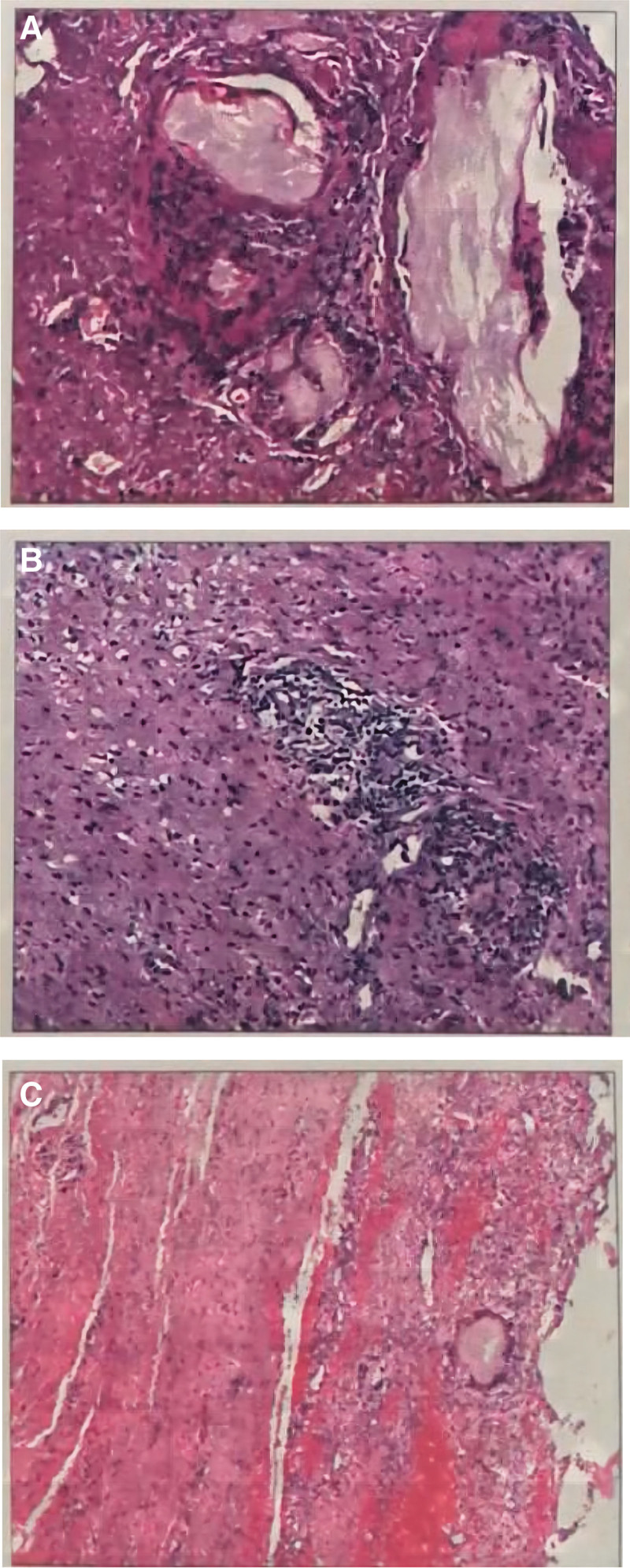
Combining with lab examinations, imaging examinations, and histopathological results, the patient was diagnosed with lumbar spinal canal tophi.
After active improvement of all examinations, the patient underwent surgical treatment with decompression and internal fixation of the L4-L5 segment.
After surgery, the patient's symptoms improved and muscle strength returned to normal. Among the 95 previously reported patients with lumbar gout, the ratio of men to women was 2.96:1, and the peak age group of incidence was 56 to 65 years. The onset of the disease was mainly in a single segment of the lumbar spine, with 34.41% of all cases occurring at the L4-L5 level. 61.05% of the patients had a history of gout attacks or hyperuricemia, and the most frequently involved site was the foot and ankle, followed by the wrist. Sixty-seven patients underwent surgical treatment, and 22 chose conservative treatment, with overall satisfactory results.
The incidence of lumbar gout is low and relatively rare in the clinic and pathological biopsy is still the gold standard. Vertebral plate incision and decompression are often selected for surgical treatment, and whether to perform fusion should be comprehensively considered for the destruction of vertebral bone by gout and the reasonable selection of the extent of surgical resection. Whether choosing surgical treatment or conservative therapy, the control of uric acid levels should be emphasized.
脊椎和附件的痛风在临床上很少见,也容易误诊,我们报告了一例因腰椎椎管内痛风结石导致神经根受压的患者。
一名 51 岁男性因腰痛伴左下肢麻木 6 个多月入院。体检时,L4-S1 棘突处有压痛和叩击痛。直腿抬高试验:左侧 50°阳性。实验室检查显示 sUA 为 669 μmol/L,腰椎 MRI 显示 L4-L5 椎管内可见囊性 T1WI 低信号和 T2WI 混杂高信号影。
结合实验室检查、影像学检查和组织病理学结果,患者被诊断为腰椎椎管内痛风石。
在所有检查得到积极改善后,患者接受了 L4-L5 节段减压内固定的手术治疗。
手术后,患者症状改善,肌力恢复正常。在之前报告的 95 例腰椎痛风患者中,男女比例为 2.96:1,发病高峰年龄组为 56-65 岁。疾病主要发生在单个腰椎节段,其中 34.41%发生在 L4-L5 水平。61.05%的患者有痛风发作或高尿酸血症病史,最常受累的部位是足和踝关节,其次是手腕。67 例患者接受了手术治疗,22 例选择了保守治疗,总体效果满意。
腰椎痛风发病率低,在临床上较为少见,病理活检仍是金标准。手术治疗常选择椎板切开减压,应根据痛风对椎骨的破坏和手术切除范围的合理选择,综合考虑是否进行融合。无论是选择手术治疗还是保守治疗,都应强调控制尿酸水平。