Faculty of Pharmacy, University of Montreal, Case Postale 6128, Succursale Centre-Ville, Montreal, QC, Canada.
Chaire Sanofi sur l'Utilisation des Médicaments de l'Université de Montréal, Montreal, Canada.
Sci Rep. 2022 Nov 19;12(1):19963. doi: 10.1038/s41598-022-24285-4.
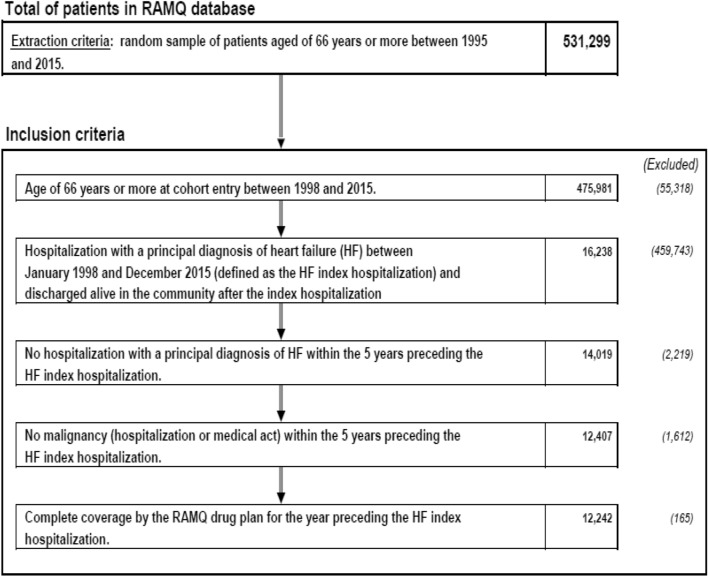
Heart failure (HF) is associated with morbidity, rehospitalization and polypharmacy. The incidence rate of mortality in HF patients with polypharmacy is poorly studied. We examine the association of polypharmacy with mortality risk in incident hospitalized HF patients with a primary diagnosis after discharge from the hospital using Quebec administrative databases, Canada from 1999 to 2015. Polypharmacy, cardiovascular (CV) polypharmacy and non-CV polypharmacy were respectively defined as exposure to ≥ 10 drugs, ≥ 5 CV drugs and ≥ 5 non-CV drugs within three months prior to the case or the control selection date. We conducted a nested case-control study to estimate rate ratios (RR) of all-cause mortality using a multivariate conditional logistic regression during one-year of follow-up. We identified 12,242 HF patients with a mean age of 81.6 years. Neither CV polypharmacy (RR 0.97, 95%CI 0.82-1.15) nor non-CV polypharmacy (RR 0.93, 95%CI 0.77-1.12) were associated with lower mortality risk. However, all polypharmacy (RR 1.31, 95%CI 1.07-1.61) showed an association with mortality risk. Myocardial infarction, valvular disease, peripheral artery disease, diabetes, major bleeding, chronic kidney disease, high comorbidity score, high Frailty score, hydralazine and spironolactone users were associated with increasing mortality risk, ranging from 15 to 61%, while use of angiotensin II inhibitors, beta-blockers, statins, anticoagulant, and antiplatelets were associated with lower risk, ranging from 23 to 32%.
心力衰竭(HF)与发病率、再住院和多药治疗有关。多药治疗的 HF 患者的死亡率发生率研究甚少。我们使用加拿大魁北克省的行政数据库,在 1999 年至 2015 年期间,对出院后因原发性 HF 住院的患者,检查多药治疗与死亡率风险的相关性。多药治疗、心血管(CV)多药治疗和非 CV 多药治疗分别定义为在病例或对照选择日期前三个月内暴露于≥10 种药物、≥5 种 CV 药物和≥5 种非 CV 药物。我们进行了嵌套病例对照研究,以在一年的随访期间使用多变量条件逻辑回归来估计全因死亡率的比率比(RR)。我们确定了 12242 名平均年龄为 81.6 岁的 HF 患者。CV 多药治疗(RR0.97,95%CI0.82-1.15)和非 CV 多药治疗(RR0.93,95%CI0.77-1.12)均与较低的死亡率风险无关。然而,所有多药治疗(RR1.31,95%CI1.07-1.61)均与死亡率风险相关。心肌梗死、瓣膜病、外周动脉疾病、糖尿病、大出血、慢性肾脏病、高合并症评分、高衰弱评分、肼屈嗪和螺内酯使用者的死亡率风险增加,范围为 15%至 61%,而血管紧张素 II 抑制剂、β-受体阻滞剂、他汀类药物、抗凝剂和抗血小板药物的使用者的死亡率风险降低,范围为 23%至 32%。