School of Public Health, Xinjiang Medical University, Urumqi, China.
Department of Gastrointestinal Surgery, The Third Affiliated Hospital, Xinjiang Medical University, Urumqi, China.
Front Immunol. 2022 Nov 2;13:947802. doi: 10.3389/fimmu.2022.947802. eCollection 2022.
Increasing evidence suggests that the number of examined lymph nodes (ELNs) is strongly linked to the survivorship of gastric cancer (GC). The goal of this study was to assess the prognostic implications of the ELNs number and to construct an ELNs-based risk signature and nomogram model to predict overall survival (OS) characteristics in GC patients.
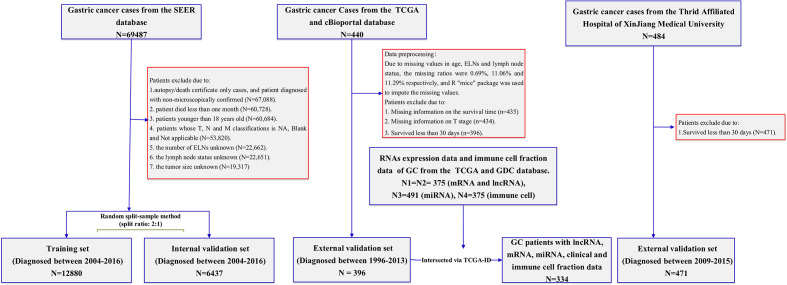
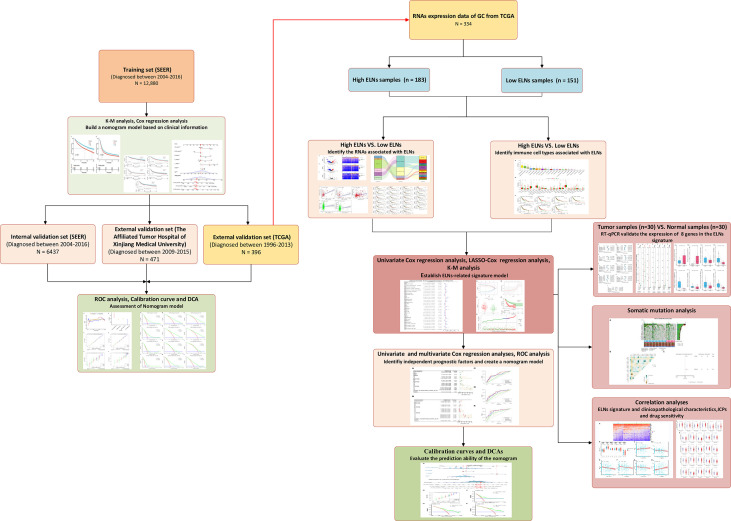
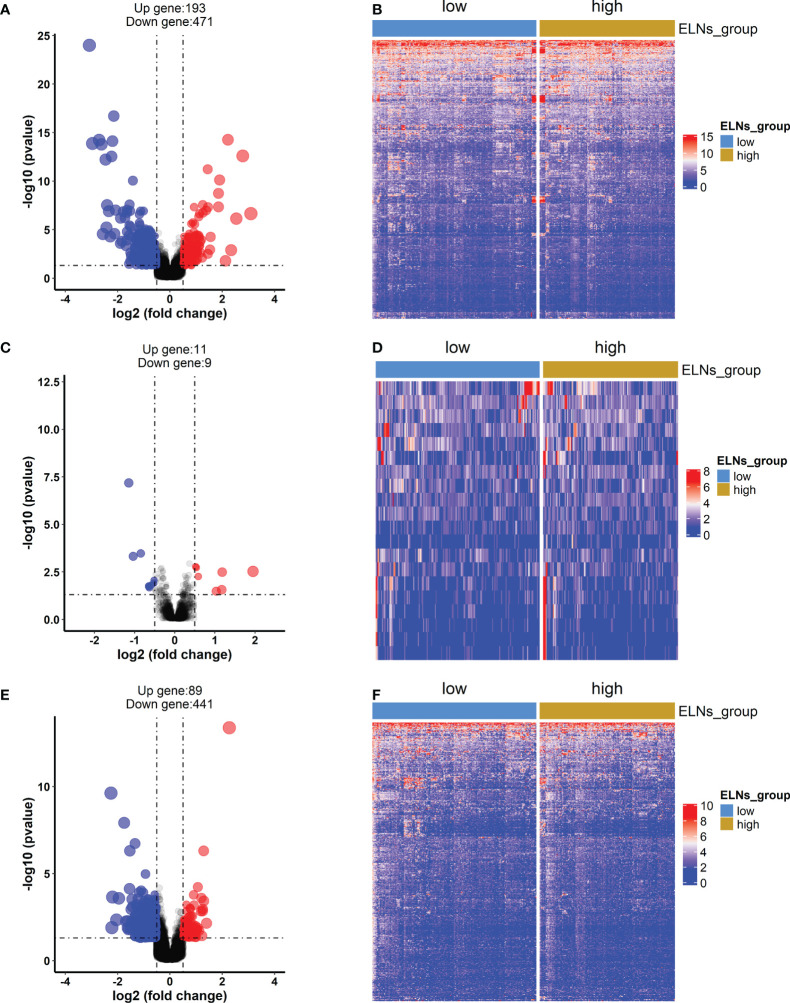
This inception cohort study included 19,317 GC patients from the U.S. Surveillance, Epidemiology, and End Results (SEER) database, who were separated into a training group and an internal validation group. The nomogram was built with the training set, then internally verified with SEER data, and externally validated with two different data sets. Based on the RNA-seq data, ELNs-related DERNAs (DElncRNAs, DEmiRNAs, andDEmRNAs) and immune cells were identified. The LASSO-Cox regression analysis was utilized to construct ELNs-related DERNAs and immune cell prognostic signature in The Cancer Genome Atlas (TCGA) cohort. The OS of subgroups with high- and low-ELN signature was compared using the Kaplan-Meier (K-M) analysis. A nomogram was successfully constructed based on the ELNs signature and other clinical characteristics. The concordance index (C-index), calibration plot, receiver operating characteristic curve, and decision curve analysis (DCA) were all used to evaluate the nomogram model. The meta-analysis, the Gene Expression Profiling Interactive Analysis database, and reverse transcription-quantitative PCR (RT-qPCR) were utilized to validate the RNA expression or abundance of prognostic genes and immune cells between GC tissues and normal gastric tissues, respectively. Finally, we analyzed the correlations between immune checkpoints, chemotherapy drug sensitivity, and risk score.
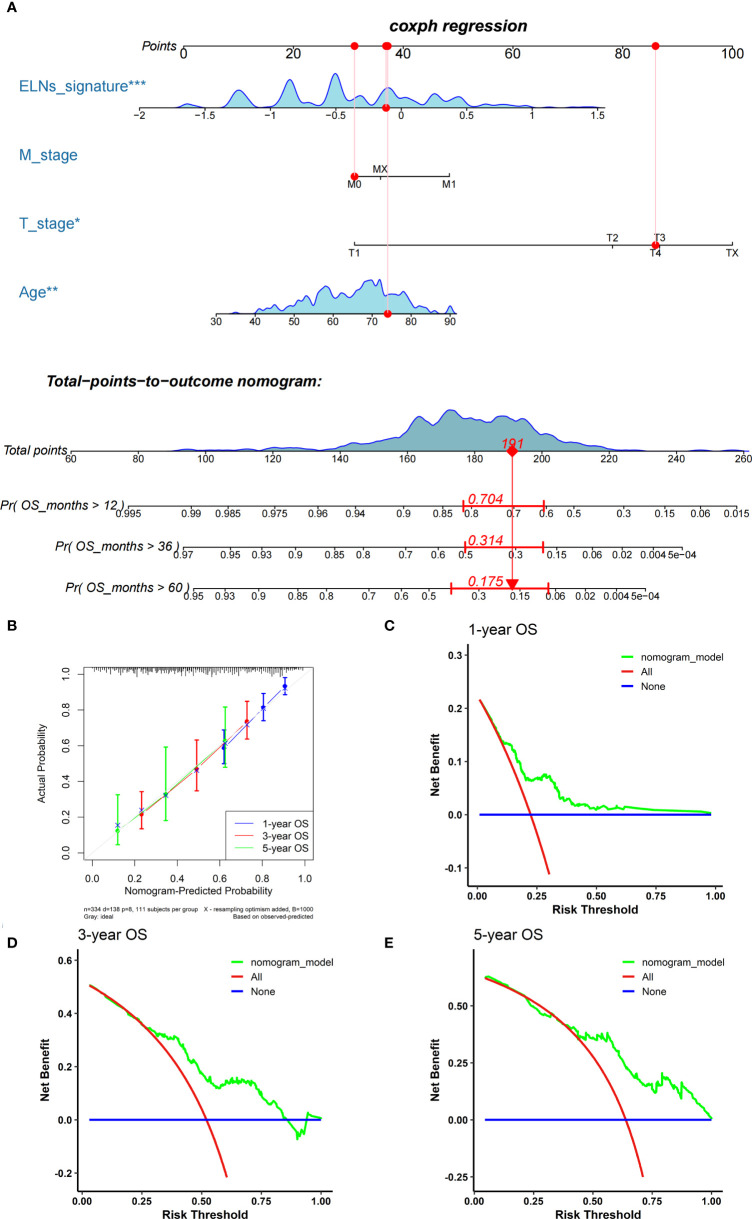
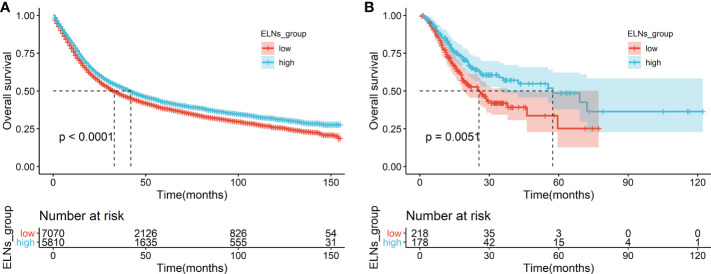
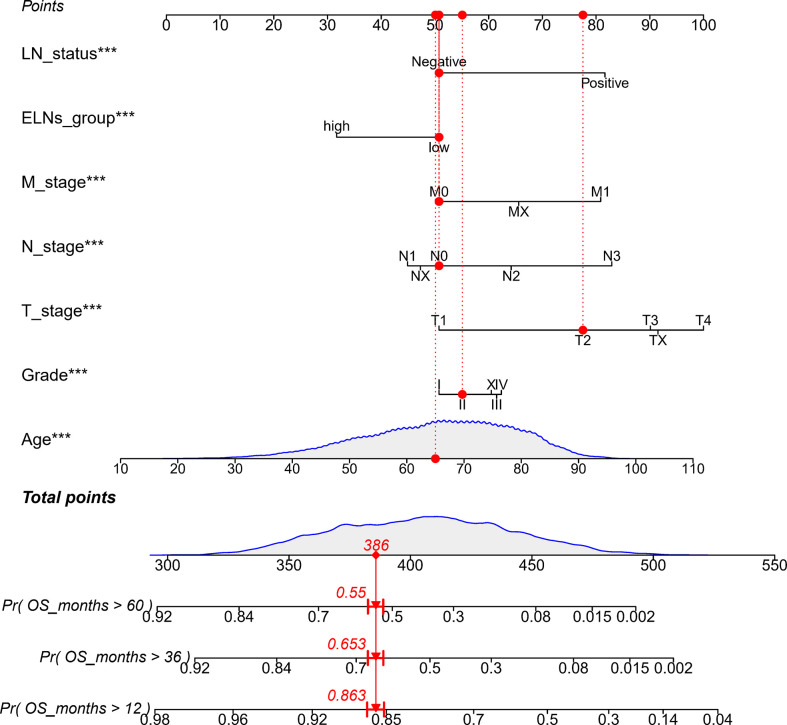
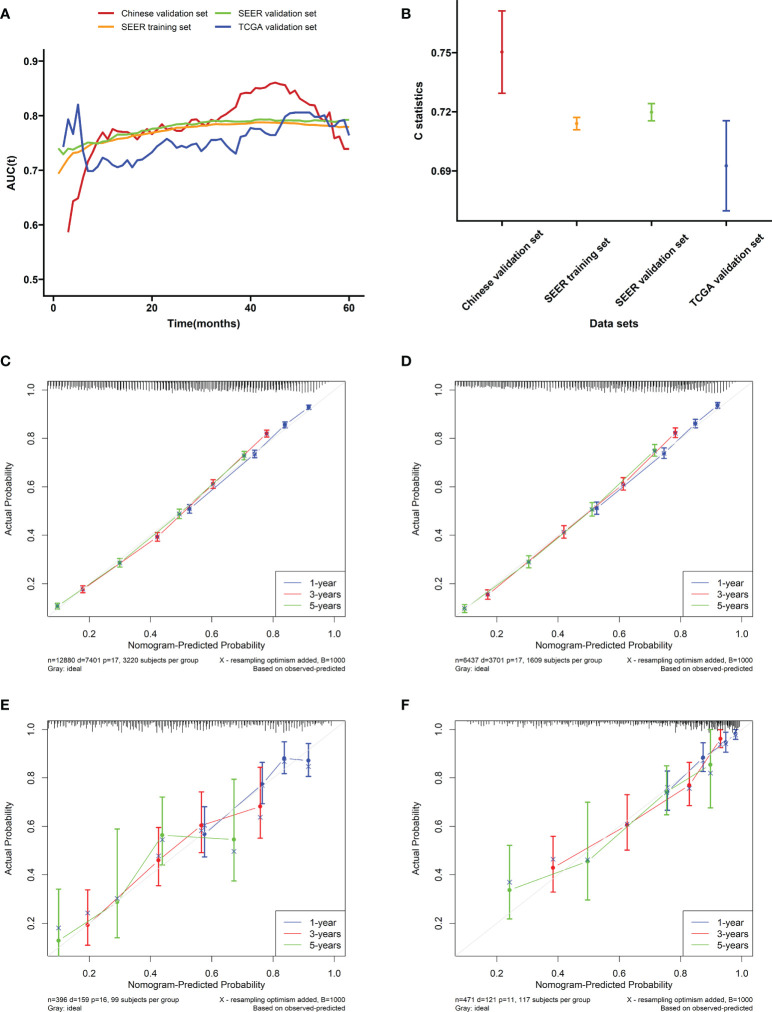
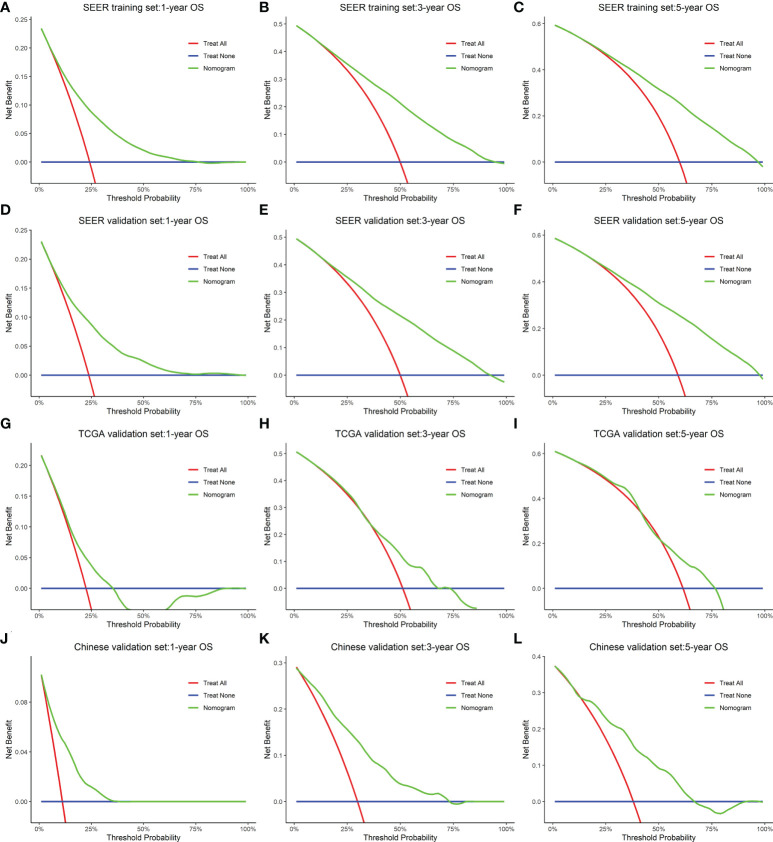
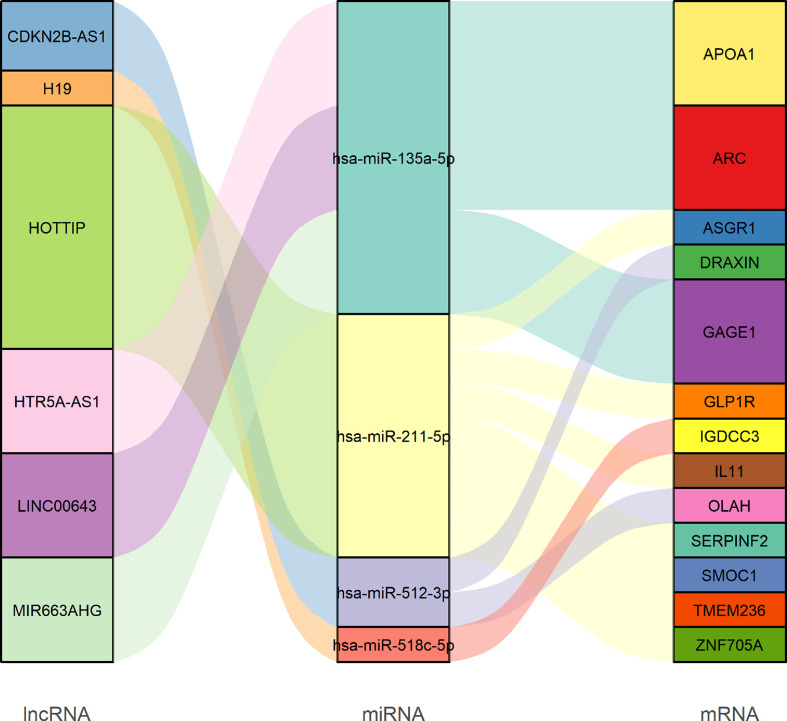
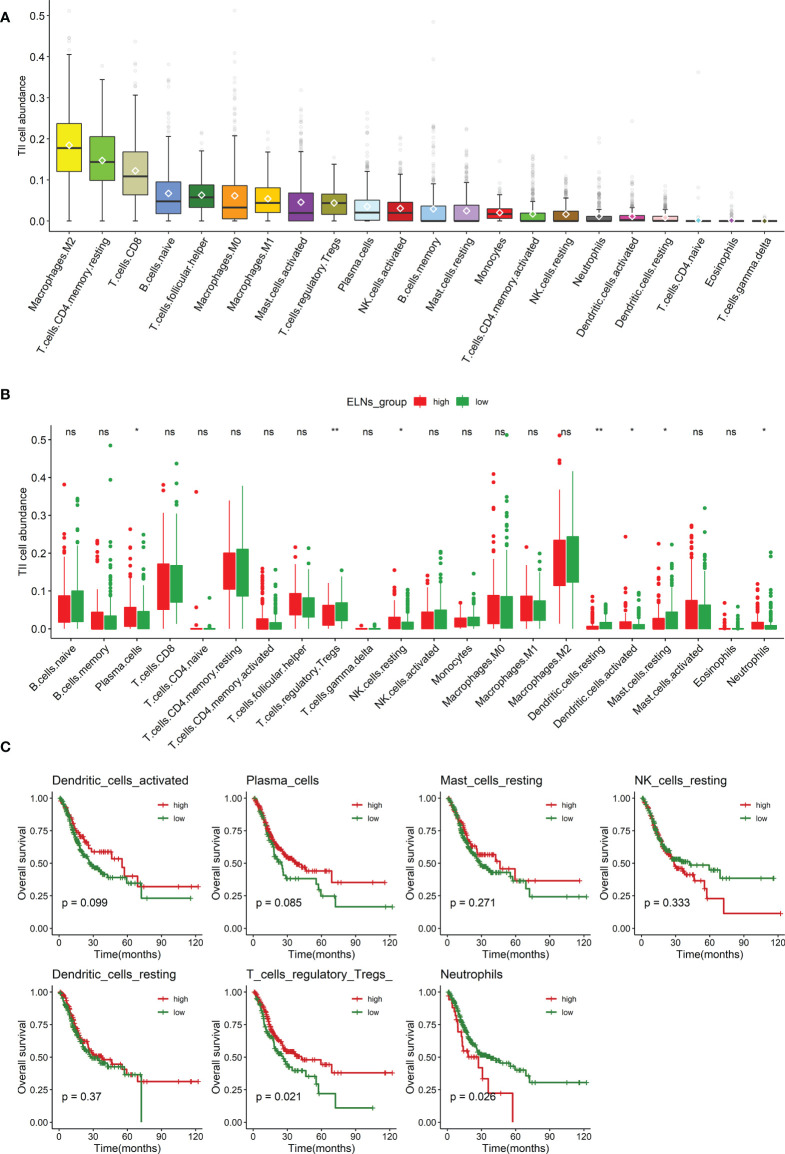
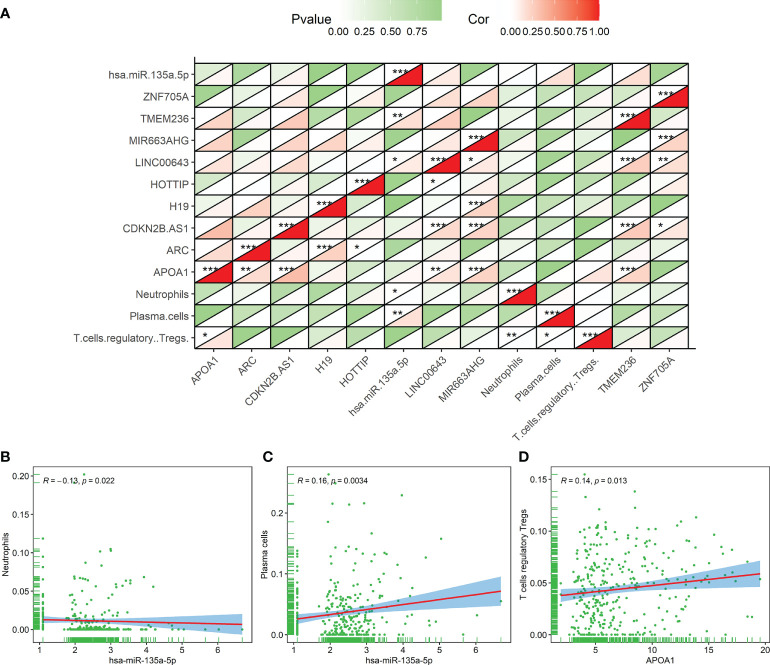
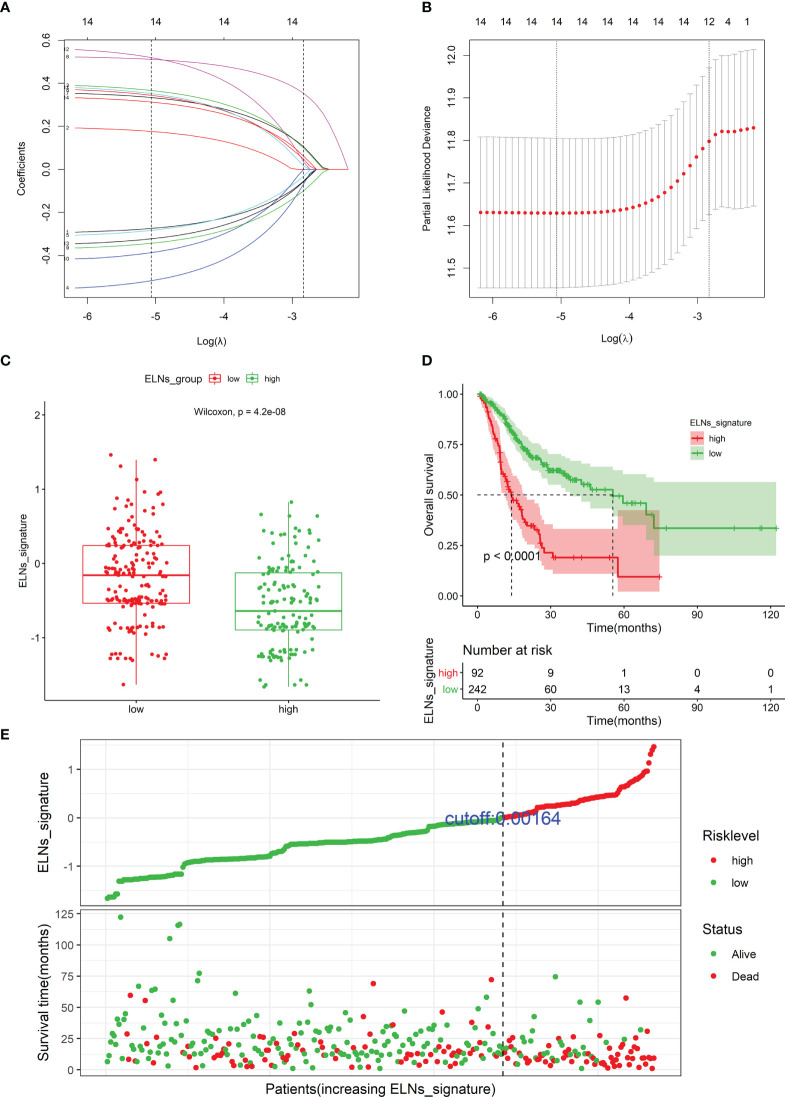
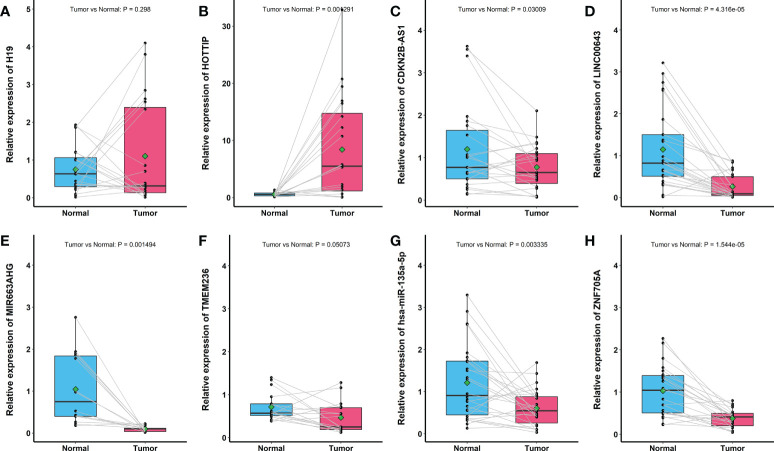
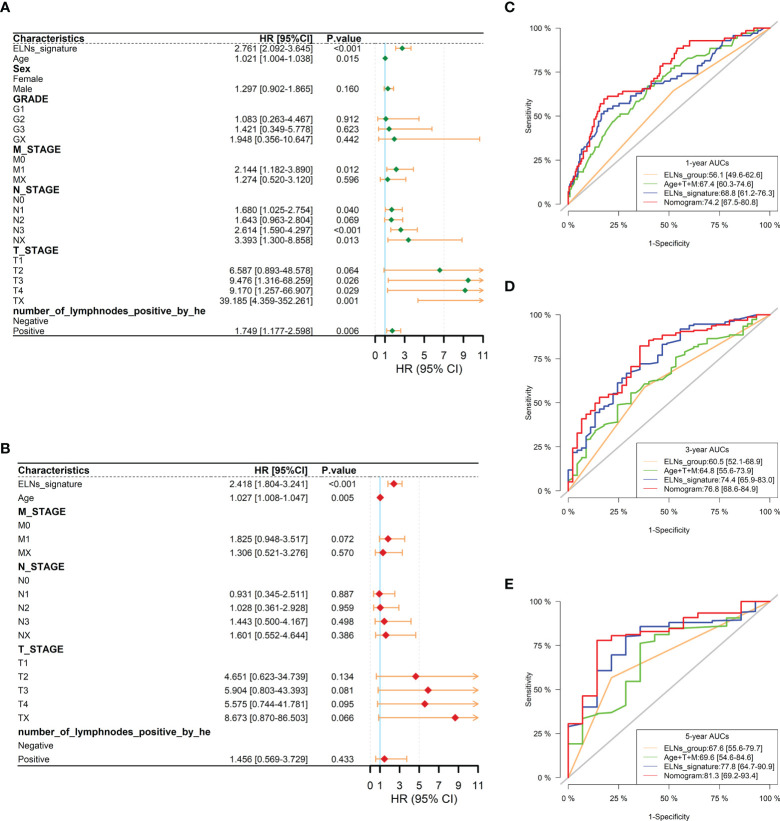
The multivariate analysis revealed that the high ELNs improved OS compared with low ELNs (hazard ratio [HR] = 0.659, 95% confidence interval [CI]: 0.626-0.694, p < 0.0001). Using the training set, a nomogram incorporating ELNs was built and proven to have good calibration and discrimination (C-index [95% CI], 0.714 [0.710-0.718]), which was validated in the internal validation set (C-index [95% CI], 0.720 [0.714-0.726]), the TCGA set (C-index [95% CI], 0.693 [0.662-0.724]), and the Chinese set (C-index [95% CI], 0.750 [0.720-0.782]). An ELNs-related signature model based on ELNs group, regulatory T cells (Tregs), neutrophils, CDKN2B-AS1, H19, HOTTIP, LINC00643, MIR663AHG, TMEM236, ZNF705A, and hsa-miR-135a-5p was constructed by the LASSO-Cox regression analysis. The result showed that OS was remarkably lower in patients with high-ELNs signature compared with those with low-ELN signature (HR = 2.418, 95% CI: 1.804-3.241, p < 0.001). This signature performed well in predicting 1-, 3-, and 5-year survival (AUC [95% CI] = 0.688 [0.612-0.763], 0.744 [0.659-0.830], and 0.778 [0.647-0.909], respectively). The multivariate Cox analysis illustrated that the risk score was an independent predictor of survival for patients with GC. Moreover, the expression of prognostic genes (LINC00643, TMEM236, and hsa-miR-135a-5p) displayed differences between GC tissues and adjacent non-tumor tissues. The C-index of the nomogram that can be used to predict the OS of GC patients was 0.710 (95% CI: 0.663-0.753). Both the calibration plots and DCA showed that the nomogram has good predictive performance. Moreover, the signature was significantly correlated with the N stage and T stage. According to our analysis, GC patients in the low-ELN signature group may have a better immunotherapy response and OS outcome.
We explored the prognostic role of ELNs in GC and successfully constructed an ELNs signature linked to the GC prognosis in TCGA. The findings manifested that the signature is a powerful predictive indicator for patients with GC. The signature might contain potential biomarkers for treatment response prediction for GC patients. Additionally, we identified a novel and robust nomogram combining the characteristics of ELNs and clinical factors for predicting 1-, 3-, and 5-year OS in GC patients, which will facilitate personalized survival prediction and aid clinical decision-making in GC patients.
越来越多的证据表明,淋巴结检查数量(ELNs)与胃癌(GC)患者的生存率密切相关。本研究旨在评估 ELNs 数量的预后意义,并构建基于 ELNs 的风险特征和列线图模型,以预测 GC 患者的总体生存(OS)特征。
这项基于队列的研究纳入了来自美国监测、流行病学和最终结果(SEER)数据库的 19317 名 GC 患者,将其分为训练组和内部验证组。列线图是利用训练集构建的,然后在 SEER 数据中进行内部验证,并在两个不同的数据集上进行外部验证。基于 RNA-seq 数据,鉴定了与 ELNs 相关的 DERNAs(DElncRNAs、DEmiRNAs 和 DEmRNAs)和免疫细胞。利用 LASSO-Cox 回归分析构建了 TCGA 队列中与 ELNs 相关的 DERNAs 和免疫细胞预后特征。使用 Kaplan-Meier(K-M)分析比较高和低 ELN 特征亚组的 OS。成功构建了基于 ELNs 特征和其他临床特征的列线图模型。一致性指数(C-index)、校准图、接收器工作特征曲线和决策曲线分析(DCA)均用于评估列线图模型。Meta 分析、基因表达谱交互分析数据库和逆转录定量 PCR(RT-qPCR)分别用于验证 GC 组织和正常胃组织之间预后基因和免疫细胞的 RNA 表达或丰度。最后,我们分析了免疫检查点、化疗药物敏感性与风险评分之间的相关性。
多因素分析显示,高 ELNs 组的 OS 明显优于低 ELNs 组(风险比[HR] = 0.659,95%置信区间[CI]:0.626-0.694,p < 0.0001)。利用训练集构建了一个包含 ELNs 的列线图,并证明其具有良好的校准度和区分度(C 指数[95%CI],0.714 [0.710-0.718]),在内部验证集(C 指数[95%CI],0.720 [0.714-0.726])、TCGA 集(C 指数[95%CI],0.693 [0.662-0.724])和中国集(C 指数[95%CI],0.750 [0.720-0.782])中得到验证。通过 LASSO-Cox 回归分析构建了基于 ELNs 组、调节性 T 细胞(Tregs)、中性粒细胞、CDKN2B-AS1、H19、HOTTIP、LINC00643、MIR663AHG、TMEM236、ZNF705A 和 hsa-miR-135a-5p 的 ELNs 相关特征模型。结果显示,高 ELNs 特征组的 OS 明显低于低 ELNs 特征组(HR = 2.418,95%CI:1.804-3.241,p < 0.001)。该特征模型在预测 1、3 和 5 年生存率方面表现良好(AUC[95%CI] = 0.688 [0.612-0.763]、0.744 [0.659-0.830]和 0.778 [0.647-0.909])。多因素 Cox 分析表明,风险评分是 GC 患者生存的独立预测因素。此外,预后基因(LINC00643、TMEM236 和 hsa-miR-135a-5p)的表达在 GC 组织和相邻非肿瘤组织之间存在差异。可用于预测 GC 患者 OS 的列线图的 C 指数为 0.710(95%CI:0.663-0.753)。校准图和 DCA 均显示该列线图具有良好的预测性能。此外,该特征与 N 分期和 T 分期显著相关。根据我们的分析,低 ELNs 特征组的 GC 患者可能具有更好的免疫治疗反应和 OS 结局。
我们探讨了 ELNs 在 GC 中的预后作用,并成功构建了一个与 TCGA 中 GC 预后相关的基于 ELNs 的特征。研究结果表明,该特征是 GC 患者强有力的预测指标。该特征可能包含用于预测 GC 患者治疗反应的潜在生物标志物。此外,我们还确定了一种新的稳健列线图,该列线图结合了 ELNs 特征和临床因素,可用于预测 GC 患者 1、3 和 5 年 OS,这将有助于个性化生存预测,并为 GC 患者的临床决策提供支持。