Section of Cardiology, Department of Medicine, University of Verona, Piazzale A. Stefani 1, 37126, Verona, Italy.
Department of Medical Biotechnologies, Division of Cardiology, University of Siena, Siena, Italy.
Int J Cardiovasc Imaging. 2022 Dec;38(12):2635-2644. doi: 10.1007/s10554-022-02669-x. Epub 2022 Jul 1.
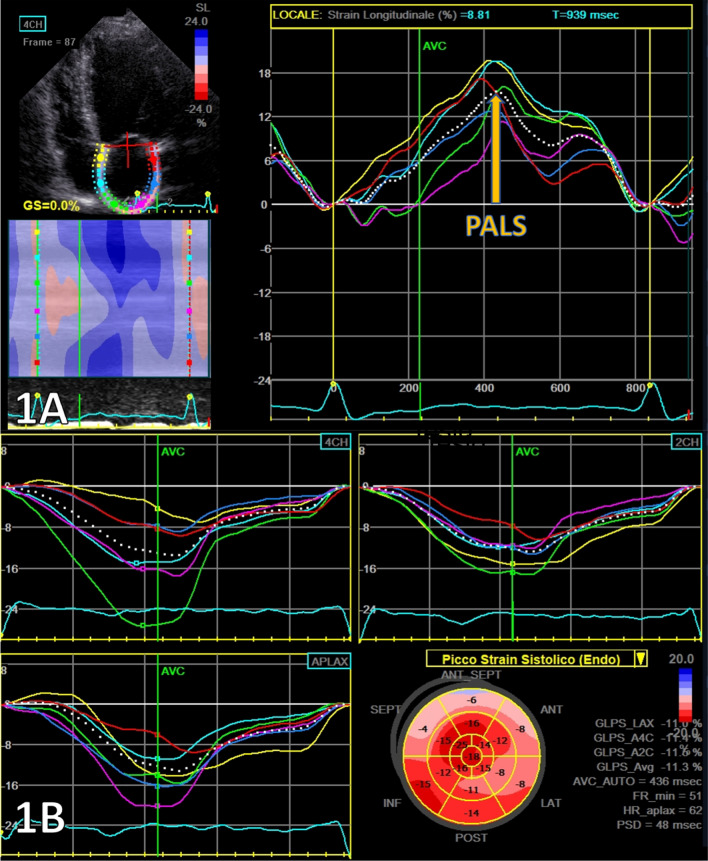
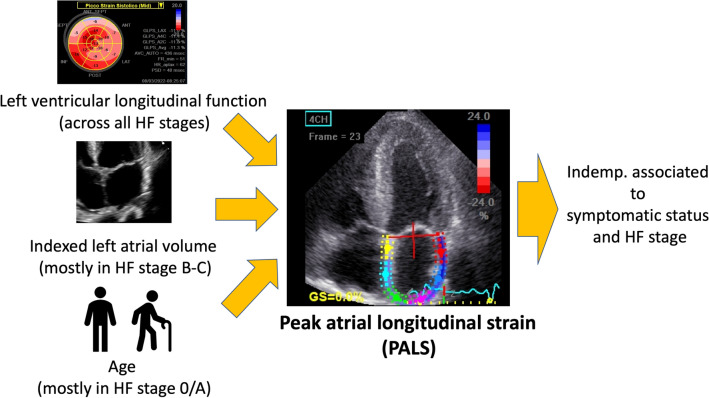
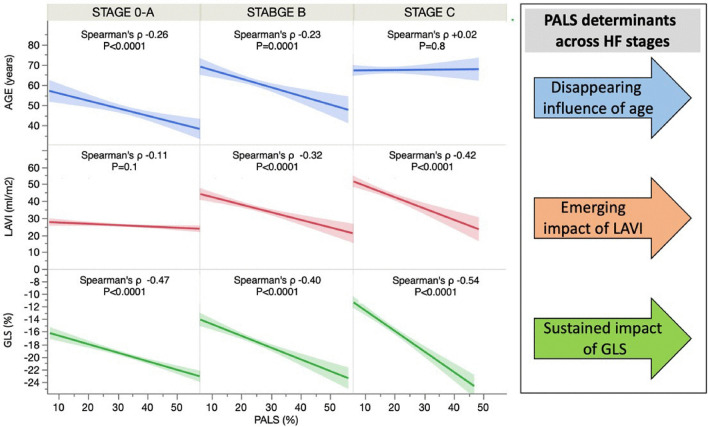
Few studies analyzed left atrial (LA) peak atrial longitudinal strain (PALS) determinants, particularly across heart failure (HF) stages. We aimed to analyze the pathophysiological and clinical PALS correlates in a large multicentric prospective study. This is a multicenter prospective observational study enrolling 745 patients with HF stages. Data included PALS and left ventricular global longitudinal strain (LV-GLS). Exclusion criteria were: valvular prosthesis; atrial fibrillation; cardiac transplantation; poor acoustic window. Median global PALS was 17% [24-32]. 29% of patients were in HF-stage 0/A, 35% in stage-B, and 36% in stage-C. Together with age, the echocardiographic determinants of PALS were LA volume and LV-GLS (overall model R = 0.50, p < 0.0001). LV-GLS had the strongest association with PALS at multivariable analysis (beta: -3.60 ± 0.20, p < 0.0001). Among HF stages, LV-GLS remained the most important PALS predictor (p < 0.0001) whereas age was only associated with PALS in lower HF-stage 0/A or B (R = - 0.26 p < 0.0001, R = - 0.23 p = 0.0001). LA volume increased its association to PALS moving from stage 0/A (R = - 0.11; P = 0.1) to C (R = - 0.42; P < 0.0001). PALS was the single most potent echocardiographic parameter in predicting the HF stage (AUC for B vs. 0/A 0.81, and AUC vs. 0/A for C 0.76). PALS remained independently associated with HF stages after adjusting for ejection fraction, E/e' ratio, and mitral regurgitation grade (p < 0.0001). Although influenced by LV-GLS and LA size across HF stages, PALS is incrementally and independently associated with clinical status. LA function may reflect a substantial part of the hemodynamic consequences of ventricular dysfunction.
很少有研究分析左心房(LA)峰值心房纵向应变(PALS)的决定因素,特别是在心力衰竭(HF)各个阶段。我们旨在通过一项大型多中心前瞻性研究来分析 PALS 的病理生理和临床相关性。这是一项多中心前瞻性观察性研究,共纳入 745 名 HF 分期患者。数据包括 PALS 和左心室整体纵向应变(LV-GLS)。排除标准为:人工瓣膜;心房颤动;心脏移植;超声图像质量差。中位整体 PALS 为 17%[24-32]。29%的患者为 HF 阶段 0/A,35%为阶段 B,36%为阶段 C。与年龄一起,PALS 的超声心动图决定因素为左心房容积和 LV-GLS(整体模型 R=0.50,p<0.0001)。多变量分析中,LV-GLS 与 PALS 的相关性最强(β:-3.60±0.20,p<0.0001)。在 HF 各阶段中,LV-GLS 仍然是 PALS 最重要的预测因子(p<0.0001),而年龄仅与 HF 阶段 0/A 或 B 中 PALS 相关(R=-0.26,p<0.0001,R=-0.23,p=0.0001)。LA 容积从 HF 阶段 0/A(R=-0.11;P=0.1)到 C(R=-0.42;P<0.0001)时,与 PALS 的相关性增加。PALS 是预测 HF 阶段的最有力的超声心动图参数(B 与 0/A 的 AUC 为 0.81,C 与 0/A 的 AUC 为 0.76)。在调整射血分数、E/e'比值和二尖瓣反流程度后,PALS 与 HF 阶段仍独立相关(p<0.0001)。尽管 PALS 在 HF 各阶段受到 LV-GLS 和 LA 大小的影响,但它与临床状态仍呈递增且独立相关。LA 功能可能反映了心室功能障碍的血流动力学后果的重要部分。