Department of Health Policy and Management, School of Public Health, Peking University, Beijing, China.
Division of Health Statistics, Centre for Health Statistics and Information, National Health Commission of China, Beijing, China
BMJ Glob Health. 2022 Nov;7(11). doi: 10.1136/bmjgh-2022-010552.
We comprehensively evaluate whether the Chinese Government's goal of ensuring Universal Health Coverage for essential health services has been achieved.
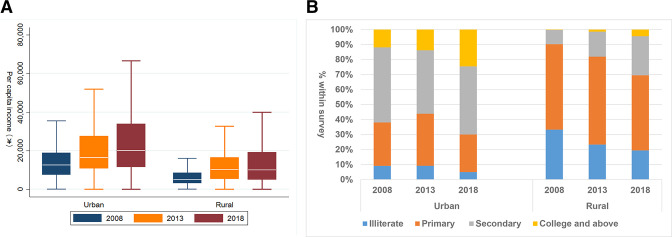
We used data from the 2008, 2013 and 2018 National Health Services Survey to report on the coverage of a range of Sustainable Development Goals (SDG) indicator 3.8.1. We created per capita household income deciles for urban and rural samples separately. We report time trends in coverage and the slope index (SII) and relative index (RII).
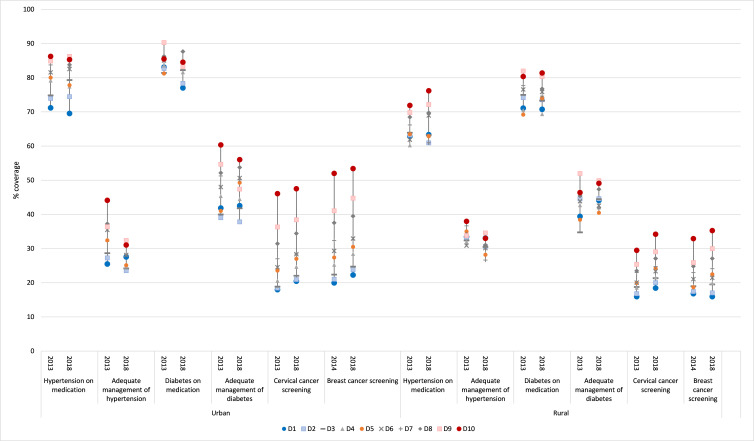
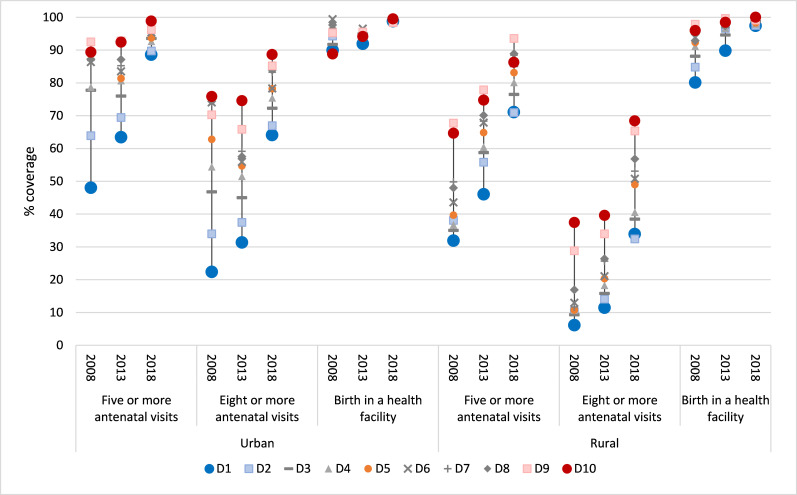
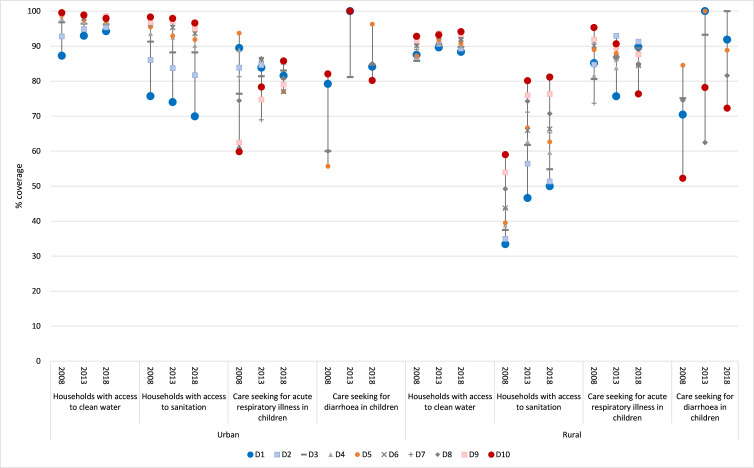
Despite much lower levels of income and education, rural populations made as much progress as their urban counterparts for most interventions. Coverage of maternal and child health interventions increased substantially in urban and rural areas, with decreasing rich-poor inequalities except for antenatal care. In rural China, one-fifth women could not access 5 or more antenatal visits. Coverage of 8 or more visits were 34% and 68%, respectively in decile D1 (the poorest) and decile D10 (the richest) (SII 35% (95% CI 22% to 48%)). More than 90% households had access to clean water, but basic sanitation was poor for rural households and the urban poorest, presenting bottom inequality. Effective coverage for non-communicable diseases was low. Medication for hypertension and diabetes were relatively high (>70%). But adequate management, counting in preventive interventions, were much lower and decreased overtime, although inequalities were small in size. Screening of cervical and breast cancer was low in both urban and rural areas, seeing no progress overtime. Cervical cancer screening was only 29% (urban) and 24% (rural) in 2018, presenting persisted top inequalities (SII 25% urban, 14% rural).
China has made commendable progress in protecting the poorest for basic care. However, the 'leaving no one behind' agenda needs a strategy targeting the entire population rather than only the poorest. Blunt investing in primary healthcare facilities seems neither effective nor efficient.
本研究全面评估了中国政府确保全民享有基本医疗卫生服务的目标是否已经实现。
我们使用了 2008 年、2013 年和 2018 年国家卫生服务调查的数据,报告了可持续发展目标(SDG)指标 3.8.1 的一系列指标的覆盖情况。我们分别为城市和农村样本创建了人均家庭收入十分位数。我们报告了覆盖范围的时间趋势以及斜率指数(SII)和相对指数(RII)。
尽管农村地区的收入和教育水平较低,但大多数干预措施的农村人口取得的进展与城市人口相当。城乡地区母婴健康干预措施的覆盖面大幅增加,除了产前护理之外,贫富差距逐渐缩小。在中国农村,有五分之一的妇女无法获得 5 次或更多次产前检查。在十分位数 D1(最贫穷)和十分位数 D10(最富裕)中,分别有 34%和 68%的妇女接受了 8 次或更多次产前检查(SII 为 35%(95%CI 22%至 48%))。超过 90%的家庭能够获得清洁用水,但农村家庭和城市最贫困家庭的基本卫生条件较差,呈现出最底层的不平等。非传染性疾病的有效覆盖率较低。高血压和糖尿病药物的使用率相对较高(>70%)。但适当的管理,包括预防干预措施,要低得多,并且随着时间的推移而减少,尽管不平等的规模较小。城乡地区的宫颈癌和乳腺癌筛查都较低,随着时间的推移没有取得进展。2018 年,宫颈癌筛查在城市和农村地区的覆盖率分别为 29%(城市)和 24%(农村),呈现出持续的上层不平等(城市 SII 为 25%,农村为 14%)。
中国在保护最贫困人群获得基本医疗方面取得了值得称赞的进展。然而,“不让一个人掉队”的议程需要一项针对整个人口的战略,而不仅仅是针对最贫困的人群。在初级医疗保健设施方面的盲目投资似乎既没有效果也没有效率。