Health Services Research, Southern California University of Health Sciences, 16200 Amber Valley Drive, 90604, Whittier, CA, USA.
The Dartmouth Institute for Health Policy and Clinical Practice, Dartmouth College, Hanover, NH, USA.
BMC Geriatr. 2022 Nov 29;22(1):917. doi: 10.1186/s12877-022-03495-5.
Cervical artery dissection and subsequent ischemic stroke is the most serious safety concern associated with cervical spinal manipulation.
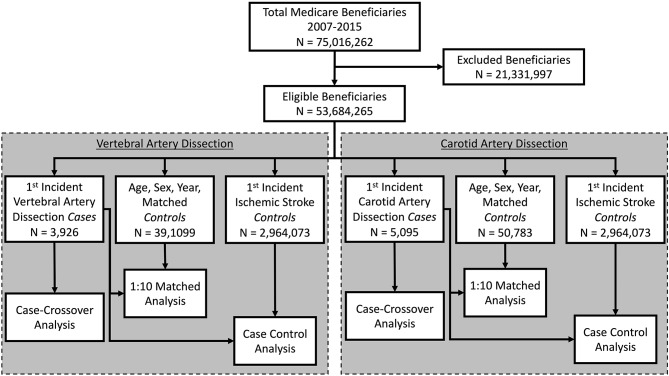
We evaluated the association between cervical spinal manipulation and cervical artery dissection among older Medicare beneficiaries in the United States. We employed case-control and case-crossover designs in the analysis of claims data for individuals aged 65+, continuously enrolled in Medicare Part A (covering hospitalizations) and Part B (covering outpatient encounters) for at least two consecutive years during 2007-2015. The primary exposure was cervical spinal manipulation; the secondary exposure was a clinical encounter for evaluation and management for neck pain or headache. We created a 3-level categorical variable, (1) any cervical spinal manipulation, 2) evaluation and management but no cervical spinal manipulation and (3) neither cervical spinal manipulation nor evaluation and management. The primary outcomes were occurrence of cervical artery dissection, either (1) vertebral artery dissection or (2) carotid artery dissection. The cases had a new primary diagnosis on at least one inpatient hospital claim or primary/secondary diagnosis for outpatient claims on at least two separate days. Cases were compared to 3 different control groups: (1) matched population controls having at least one claim in the same year as the case; (2) ischemic stroke controls without cervical artery dissection; and (3) case-crossover analysis comparing cases to themselves in the time period 6-7 months prior to their cervical artery dissection. We made each comparison across three different time frames: up to (1) 7 days; (2) 14 days; and (3) 30 days prior to index event.
The odds of cervical spinal manipulation versus evaluation and management did not significantly differ between vertebral artery dissection cases and any of the control groups at any of the timepoints (ORs 0.84 to 1.88; p > 0.05). Results for carotid artery dissection cases were similar.
Among Medicare beneficiaries aged 65 and older who received cervical spinal manipulation, the risk of cervical artery dissection is no greater than that among control groups.
颈椎动脉夹层和由此导致的缺血性中风是与颈椎推拿相关的最严重的安全隐患。
我们评估了美国老年医疗保险受益人中颈椎推拿与颈椎动脉夹层之间的关联性。我们采用病例对照和病例交叉设计,对 2007 年至 2015 年期间至少连续两年连续参加医疗保险 A 部分(涵盖住院治疗)和 B 部分(涵盖门诊治疗)的年龄在 65 岁及以上的个人的理赔数据进行分析。主要暴露因素是颈椎推拿;次要暴露因素是评估和管理颈部疼痛或头痛的临床治疗。我们创建了一个三分类变量,(1)任何颈椎推拿,(2)评估和管理但无颈椎推拿,(3)既无颈椎推拿也无评估和管理。主要结局是发生颈椎动脉夹层,包括(1)椎动脉夹层或(2)颈动脉夹层。病例至少有一份住院医院理赔或门诊理赔的主要/次要诊断,至少有两份单独的日子。病例与三组不同的对照组进行比较:(1)同年至少有一份理赔的匹配人群对照组;(2)无颈椎动脉夹层的缺血性中风对照组;(3)病例交叉分析,在病例发生颈椎动脉夹层前的 6-7 个月内将病例与自身进行比较。我们在三个不同的时间范围内进行了每一次比较:到(1)7 天;(2)14 天;(3)索引事件前 30 天。
在任何时间点,椎动脉夹层病例与任何对照组相比,颈椎推拿与评估和管理的比值比(ORs 0.84 至 1.88;p>0.05)没有显著差异。颈动脉夹层病例的结果相似。
在接受颈椎推拿的年龄在 65 岁及以上的医疗保险受益人中,发生颈椎动脉夹层的风险并不高于对照组。