The Biomedical Research Centre, School of Biomedical Engineering, University of British Columbia, Vancouver, BC, Canada.
Department of Medicine (Division of Respirology), University of British Columbia, Vancouver, BC, Canada.
Front Immunol. 2022 Nov 14;13:1010216. doi: 10.3389/fimmu.2022.1010216. eCollection 2022.
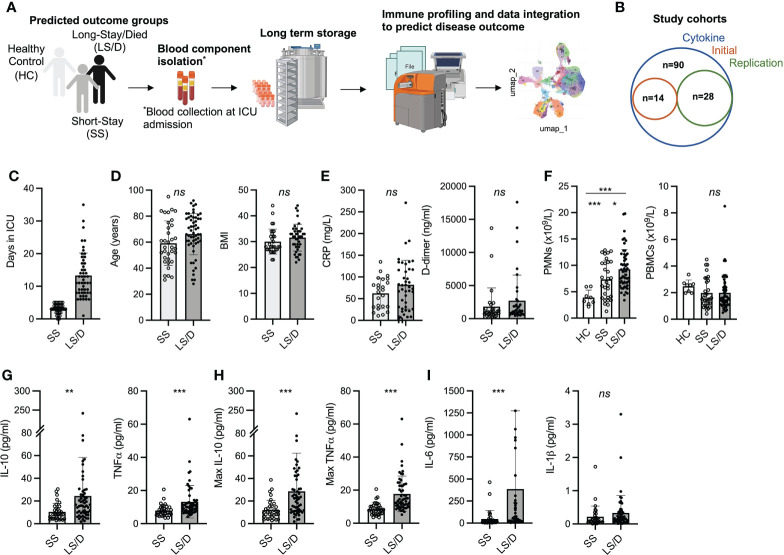
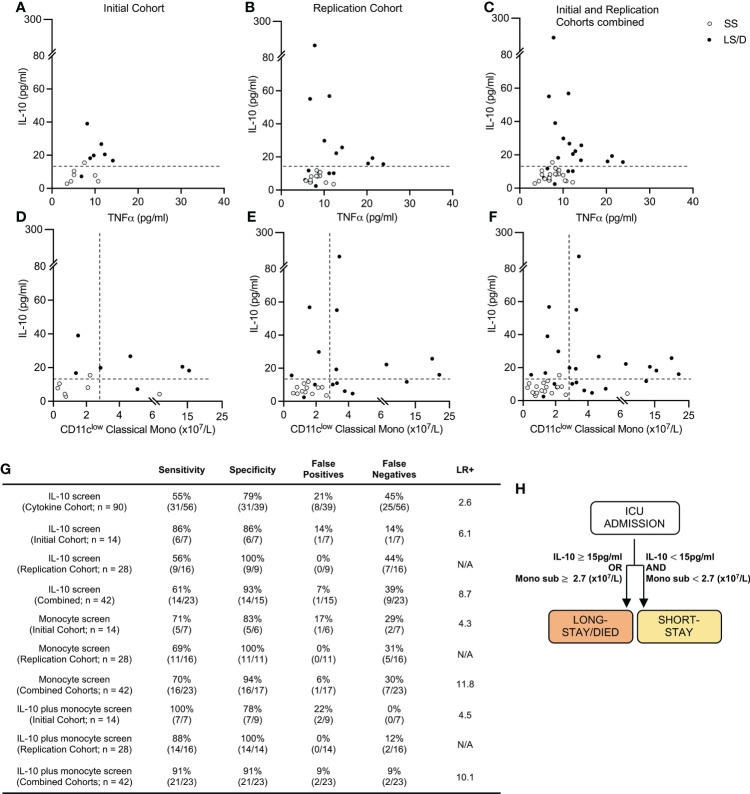
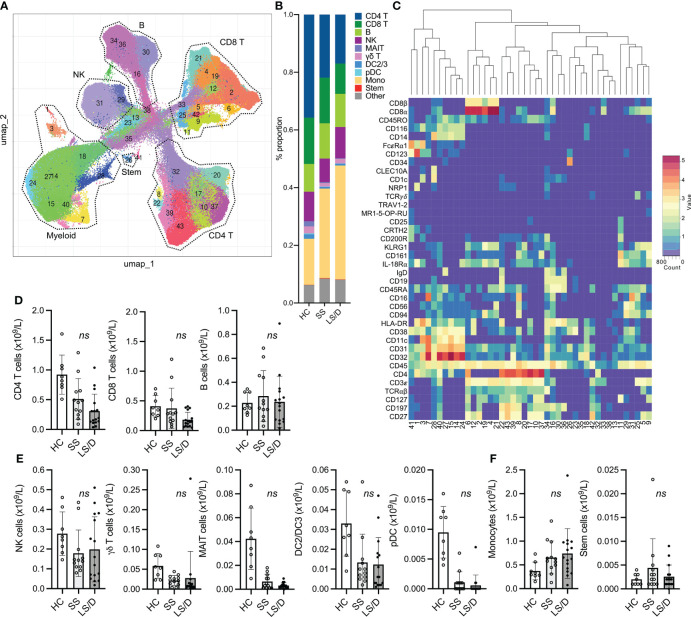
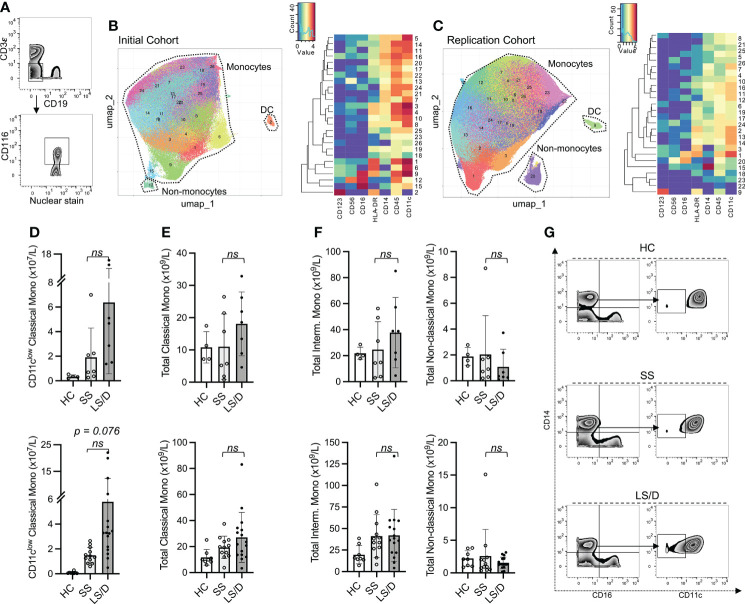
The COVID-19 pandemic continues to challenge the capacities of hospital ICUs which currently lack the ability to identify prospectively those patients who may require extended management. In this study of 90 ICU COVID-19 patients, we evaluated serum levels of four cytokines (IL-1β, IL-6, IL-10 and TNFα) as well as standard clinical and laboratory measurements. On 42 of these patients (binned into Initial and Replication Cohorts), we further performed CyTOF-based deep immunophenotyping of peripheral blood mononuclear cells with a panel of 38 antibodies. All measurements and patient samples were taken at time of ICU admission and retrospectively linked to patient clinical outcomes through statistical approaches. These analyses resulted in the definition of a new measure of patient clinical outcome: patients who will recover after short ICU stays (< 6 days) and those who will subsequently die or recover after long ICU stays (≥6 days). Based on these clinical outcome categories, we identified blood prognostic biomarkers that, at time of ICU admission, prospectively distinguish, with 91% sensitivity and 91% specificity (positive likelihood ratio 10.1), patients in the two clinical outcome groups. This is achieved through a tiered evaluation of serum IL-10 and targeted immunophenotyping of monocyte subsets, specifically, CD11c classical monocytes. Both immune biomarkers were consistently elevated ( ≥15 pg/ml and ≥2.7 x10/L for serum IL-10 and CD11c classical monocytes, respectively) in those patients who will subsequently die or recover after long ICU stays. This highly sensitive and specific prognostic test could prove useful in guiding clinical resource allocation.
COVID-19 大流行继续挑战医院 ICU 的能力,目前 ICU 缺乏前瞻性识别可能需要延长治疗的患者的能力。在这项对 90 名 ICU COVID-19 患者的研究中,我们评估了四种细胞因子(IL-1β、IL-6、IL-10 和 TNFα)的血清水平以及标准的临床和实验室测量。在其中 42 名患者(分为初始队列和复制队列)中,我们进一步使用基于 CyTOF 的外周血单核细胞进行了 38 种抗体的深度免疫表型分析。所有测量和患者样本均在 ICU 入院时采集,并通过统计方法回顾性地与患者的临床结果相关联。这些分析导致了一种新的患者临床结果衡量标准的定义:在 ICU 停留时间较短(<6 天)后康复的患者和随后在 ICU 停留时间较长(≥6 天)后死亡或康复的患者。基于这些临床结果类别,我们确定了血液预后生物标志物,在 ICU 入院时,以 91%的敏感性和 91%的特异性(阳性似然比 10.1),前瞻性地区分两组临床结果的患者。这是通过对血清 IL-10 的分层评估和单核细胞亚群(特别是 CD11c 经典单核细胞)的靶向免疫表型分析来实现的。在随后在 ICU 停留时间较长后死亡或康复的患者中,这两种免疫生物标志物均持续升高(血清 IL-10 和 CD11c 经典单核细胞分别≥15pg/ml 和≥2.7x10/L)。这种高敏感和特异性的预后测试可能有助于指导临床资源分配。