Zhang Li, Zhang Jing, Tang Min, Lei Xiao-Yan, Li Long-Chao
Department of MRI, Shaanxi Provincial People's Hospital, Xi'an 710068, China.
Institute of Medical Research, Northwestern Polytechnical University, Xi'an 710068, China.
Diagnostics (Basel). 2022 Dec 1;12(12):3005. doi: 10.3390/diagnostics12123005.
The aim of this study was to establish a predictive nomogram for predicting prostate cancer (PCa) in patients with gray-zone prostate-specific antigen (PSA) levels (4-10.0 ng/mL) based on radiomics and other traditional clinical parameters.
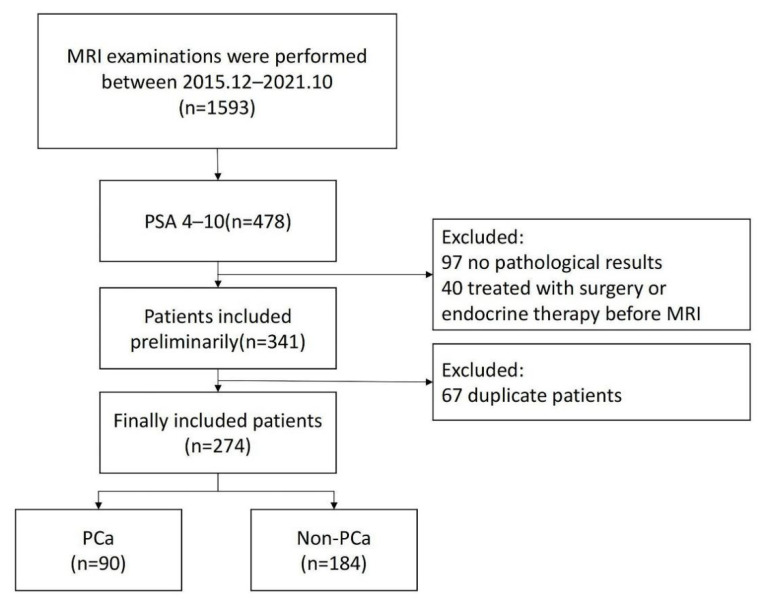
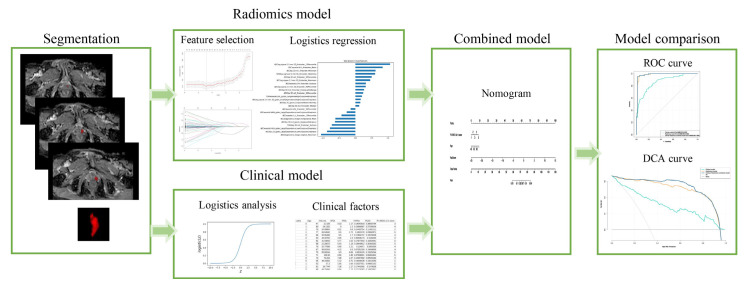
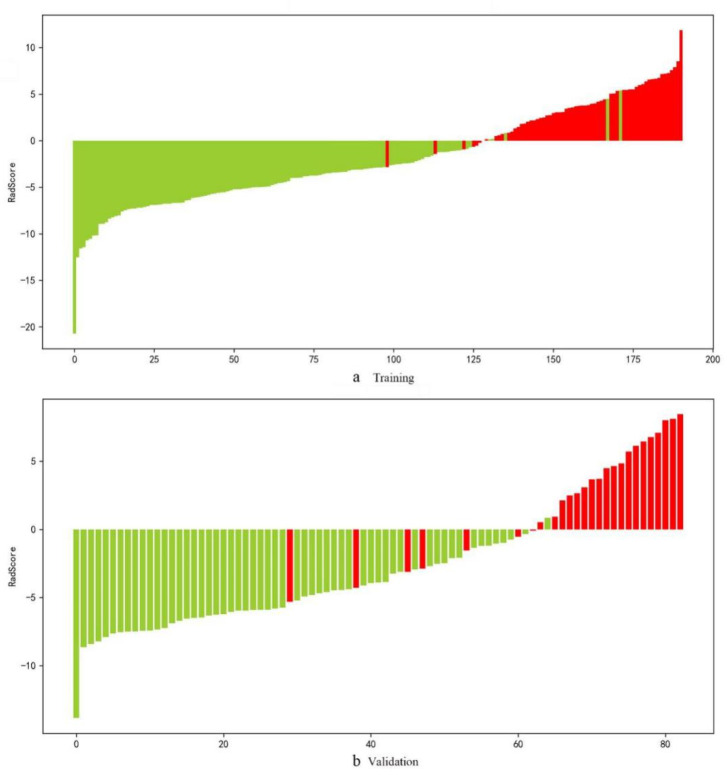
In all, 274 patients with gray-zone PSA levels were included in this retrospective study. They were randomly divided into training and validation sets (n = 191 and 83, respectively). Data on the clinical risk factors related to PCa with gray-zone PSA levels (such as Prostate Imaging Reporting and Data System, version 2.1 [PI-RADS V2.1] category, age, prostate volume, and serum PSA level) were collected for all patients. Lesion volumes of interest (VOI) from T2-weighted imaging (T2WI) and apparent diffusion coefficient (ADC) imaging were annotated by two radiologists. The radiomics model, clinical model, and combined prediction model, which was presented on a nomogram by incorporating the radiomics signature and clinical and radiological risk factors for PCa, were developed using logistic regression. The area under the receiver operator characteristic (AUC-ROC) and decision, calibration curve were used to compare the three models for the diagnosis of PCa with gray-zone PSA levels.
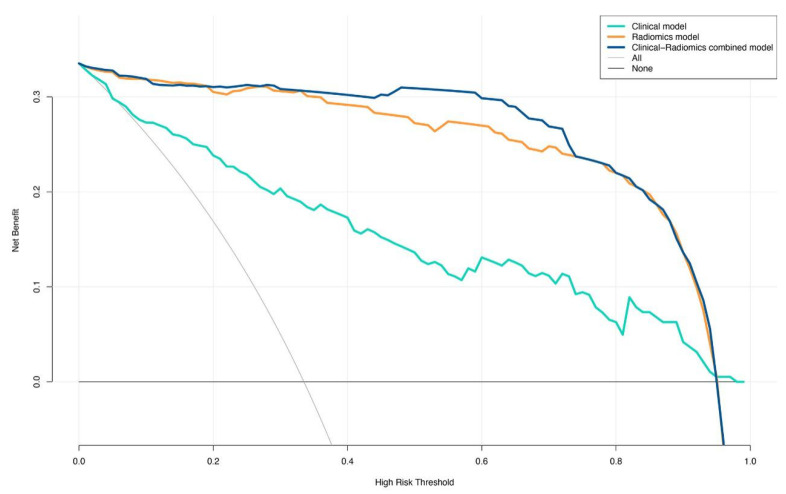
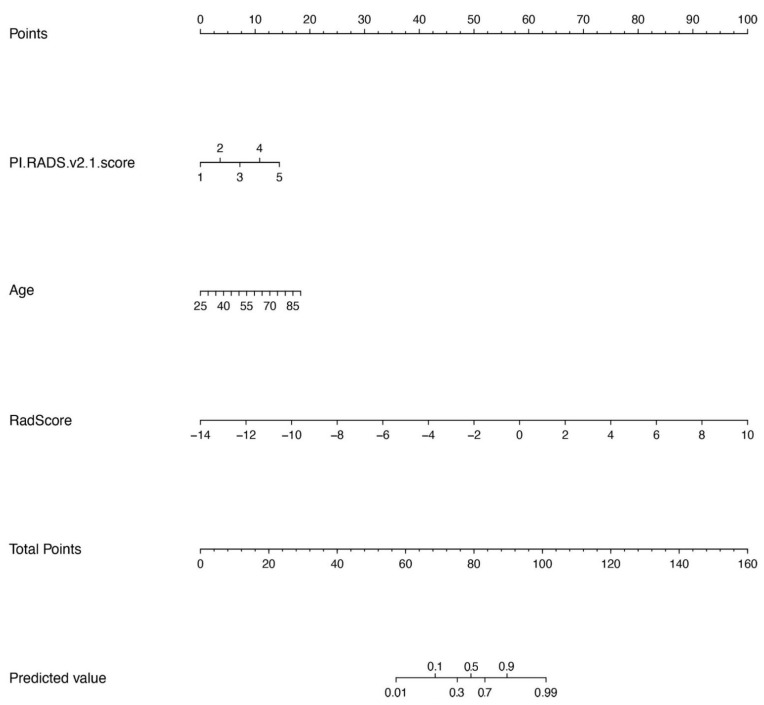
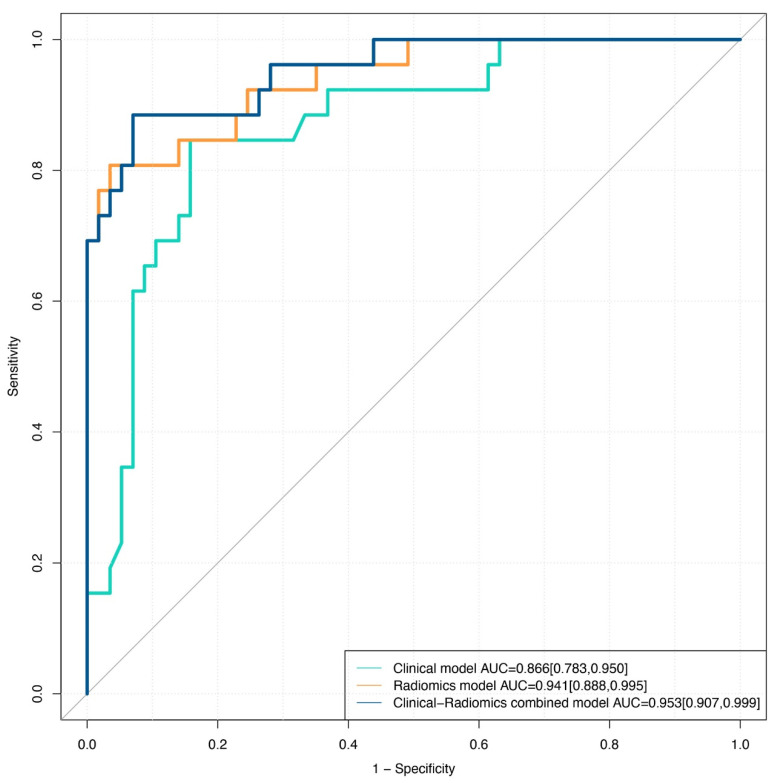
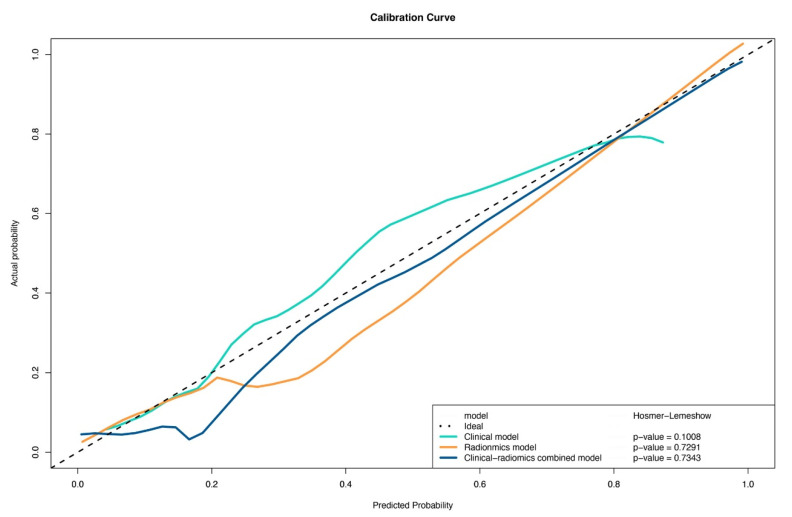
The predictive nomogram (AUC: 0.953) incorporating the radiomics score and PI-RADS V2.1 category, age, and the radiomics model (AUC: 0.941) afforded much higher diagnostic efficacy than the clinical model (AUC: 0.866). The addition of the rad score could improve the discriminatory performance of the clinical model. The decision curve analysis indicated that the radiomics or combined model could be more beneficial compared to the clinical model for the prediction of PCa. The nomogram showed good agreement for detecting PCa with gray-zone PSA levels between prediction and histopathologic confirmation.
The nomogram, which combined the radiomics score and PI-RADS V2.1 category and age, is an effective and non-invasive method for predicting PCa. Furthermore, as well as good calibration and is clinically useful, which could reduce unnecessary prostate biopsies in patients having PCa with gray-zone PSA levels.
本研究旨在基于影像组学和其他传统临床参数,建立一种预测模型,用于预测前列腺特异性抗原(PSA)处于灰色区域水平(4 - 10.0 ng/mL)的患者患前列腺癌(PCa)的风险。
本回顾性研究共纳入274例PSA处于灰色区域水平的患者。他们被随机分为训练集和验证集(分别为n = 191和83)。收集了所有患者与PSA处于灰色区域水平的PCa相关的临床危险因素数据(如前列腺影像报告和数据系统,第2.1版[PI-RADS V2.1]分类、年龄、前列腺体积和血清PSA水平)。两名放射科医生对T2加权成像(T2WI)和表观扩散系数(ADC)成像中的感兴趣病变体积(VOI)进行标注。使用逻辑回归开发了影像组学模型、临床模型以及通过整合影像组学特征与PCa的临床和放射学危险因素在列线图上呈现的联合预测模型。采用受试者操作特征曲线下面积(AUC-ROC)和决策、校准曲线来比较这三种模型对PSA处于灰色区域水平的PCa的诊断效能。
纳入影像组学评分、PI-RADS V2.1分类、年龄的预测列线图(AUC:0.953)和影像组学模型(AUC:0.941)的诊断效能远高于临床模型(AUC:0.866)。加入rad评分可提高临床模型的鉴别性能。决策曲线分析表明,与临床模型相比,影像组学或联合模型在预测PCa方面可能更具优势。列线图显示在预测和组织病理学证实之间,对于检测PSA处于灰色区域水平的PCa具有良好的一致性。
结合影像组学评分、PI-RADS V2.1分类和年龄的列线图是预测PCa的一种有效且非侵入性的方法。此外,其校准良好且具有临床实用性,可减少PSA处于灰色区域水平的PCa患者不必要的前列腺活检。