Ouzaid Idir, Rioux-Leclercq Nathalie, Khene Zine-Eddine, Bensalah Karim, Kammerer-Jacquet Solène-Florence
Department of Pathology, University of Rennes, CHU Rennes, Inserm, EHESP, Irset (Institut de recherche en santé, environnement et travail)-UMR_S1085, Rennes, France.
Department of Urology, Bichat Claude Bernard Hospital, University of Paris, Paris, France.
Eur Urol Open Sci. 2022 Dec 15;47:12-19. doi: 10.1016/j.euros.2022.11.006. eCollection 2023 Jan.
The advent of immune check inhibitors (ICIs) has tremendously changed the prognosis of metastatic renal cell carcinoma (mRCC), adding an unseen substantial overall survival benefit. These agents could be administered alone or in combination with anti-vascular endothelial growth factor (anti-VEGF) therapies. So far, treatment allocation is based only on clinical stratification risk models.
Herein, we aimed to report the different molecular classifications reported in the first-line treatment of mRCC and discuss the awaited clinical implications in terms of treatment selection.
Medline database as well as European Society for Medical Oncology (ESMO)/American Society of Clinical Oncology (ASCO) conference proceedings were searched to identify biomarker studies. Inclusion criteria comprised randomized and nonrandomized clinical trials that included patients treated in the first line of mRCC setting, patients treated with anti-VEGF therapies or ICIs, biological modeling, and available survival outcomes.
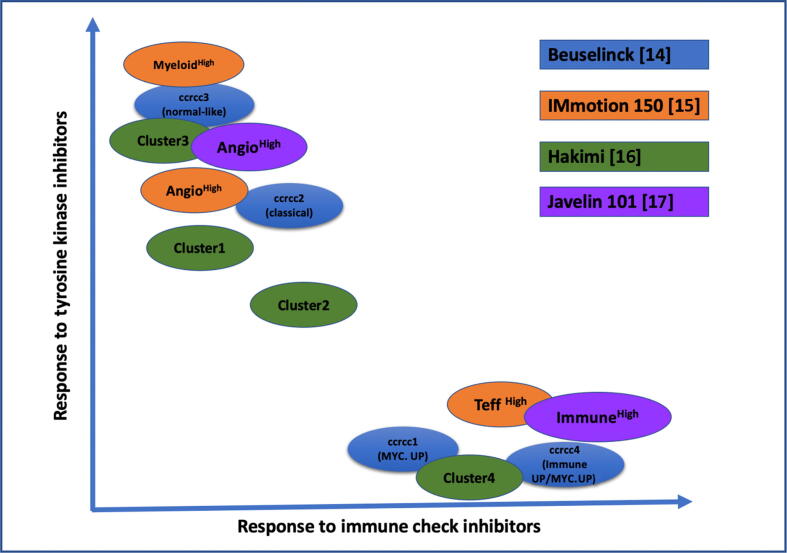
Four classification models were identified with subsequent clinical implications: Beuselinck model (34 gene signatures), IMmotion150, Hakimi, and JAVELIN 101 model. Tumor profiling shows distinct outcomes when treated with one or other combination. Patients are clustered into two gene signatures: angiogenic and proinflammatory (as per JAVELIN). The first is more likely to respond to therapy that includes anti-VEGF agents, while the best outcomes are obtained with an ICI combination with the second.
The findings presented here were mostly derived from ancillary registered studies of new drugs in the setting of mRCC. Further validation is needed, which sets new paradigms for investigation in clinical research based on tumor biology for treatment allocation and not only on clinical stratification tools.
First-line treatment of metastatic kidney includes immunotherapy alone or in combination with antiangiogenic therapy. However, clinical practice demonstrated that the "one treatment fits all" strategy might not be the best approach. In fact, recent studies showed that the addition of immunotherapy agents will not benefit all patients equally, and some still respond either equally to or better than anti-vascular endothelial growth factor alone. This review revealed biomarker modeling that impacts treatment selection. Recent tumor profiling into "angiogenic signature" more sensitive to angiogenic agents versus "immune signature" more likely to achieve the best response with immunotherapy should be validated. Tumor biology features might be more powerful than clinical classification for a tailored treatment approach.
免疫检查点抑制剂(ICI)的出现极大地改变了转移性肾细胞癌(mRCC)的预后,带来了显著的总体生存获益。这些药物可以单独使用,也可以与抗血管内皮生长因子(抗VEGF)疗法联合使用。到目前为止,治疗方案的选择仅基于临床分层风险模型。
在此,我们旨在报告mRCC一线治疗中报道的不同分子分类,并讨论在治疗选择方面有待实现的临床意义。
检索了Medline数据库以及欧洲医学肿瘤学会(ESMO)/美国临床肿瘤学会(ASCO)会议论文集,以确定生物标志物研究。纳入标准包括随机和非随机临床试验,这些试验纳入了mRCC一线治疗的患者、接受抗VEGF疗法或ICI治疗的患者、生物学建模以及可用的生存结果。
确定了四种分类模型及其后续临床意义:Beuselinck模型(34个基因特征)、IMmotion150、Hakimi和JAVELIN 101模型。肿瘤分析显示,在接受一种或另一种联合治疗时会有不同的结果。患者被分为两种基因特征:血管生成性和促炎性(根据JAVELIN)。第一种更可能对包括抗VEGF药物的治疗产生反应,而第二种与ICI联合使用可获得最佳结果。
此处呈现的研究结果大多来自mRCC背景下新药的辅助注册研究。需要进一步验证,这为基于肿瘤生物学而非仅基于临床分层工具进行治疗分配的临床研究调查设定了新的范式。
转移性肾癌的一线治疗包括单独免疫治疗或与抗血管生成治疗联合使用。然而,临床实践表明,“一刀切”的策略可能不是最佳方法。事实上,最近的研究表明,添加免疫治疗药物并不会使所有患者同等受益,而且一些患者对单独抗血管内皮生长因子的反应仍然相同或更好。本综述揭示了影响治疗选择的生物标志物建模。最近将肿瘤分析为对血管生成药物更敏感的“血管生成特征”与更可能通过免疫治疗获得最佳反应的“免疫特征”应得到验证。肿瘤生物学特征对于量身定制的治疗方法可能比临床分类更具影响力。