Department of Emergency Medicine, New York University Grossman School of Medicine, New York, New York.
Department of Psychiatry, Yale School of Medicine, New Haven, Connecticut.
JAMA Netw Open. 2022 Dec 1;5(12):e2247649. doi: 10.1001/jamanetworkopen.2022.47649.
Previous studies have demonstrated racial and ethnic inequities in medical student assessments, awards, and faculty promotions at academic medical centers. Few data exist about similar racial and ethnic disparities at the level of graduate medical education.
To examine the association between race and ethnicity and performance assessments among a national cohort of internal medicine residents.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study evaluated assessments of performance for 9026 internal medicine residents from the graduating classes of 2016 and 2017 at Accreditation Council of Graduate Medical Education (ACGME)-accredited internal medicine residency programs in the US. Analyses were conducted between July 1, 2020, and June 31, 2022.
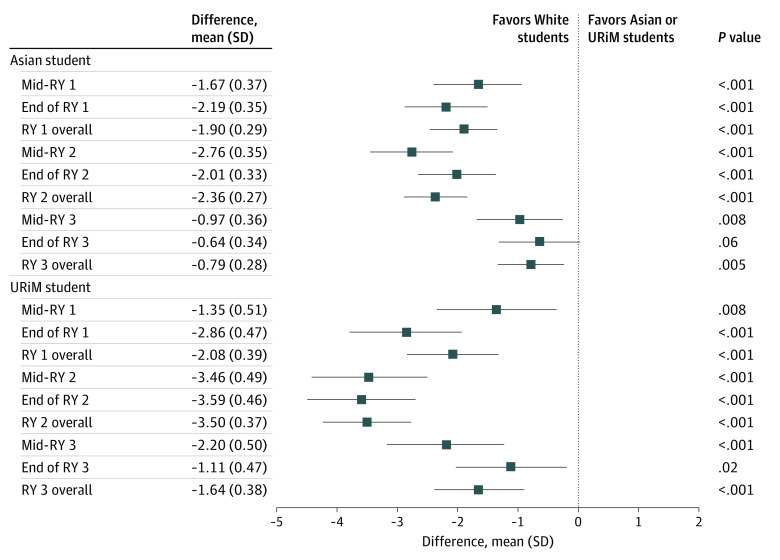
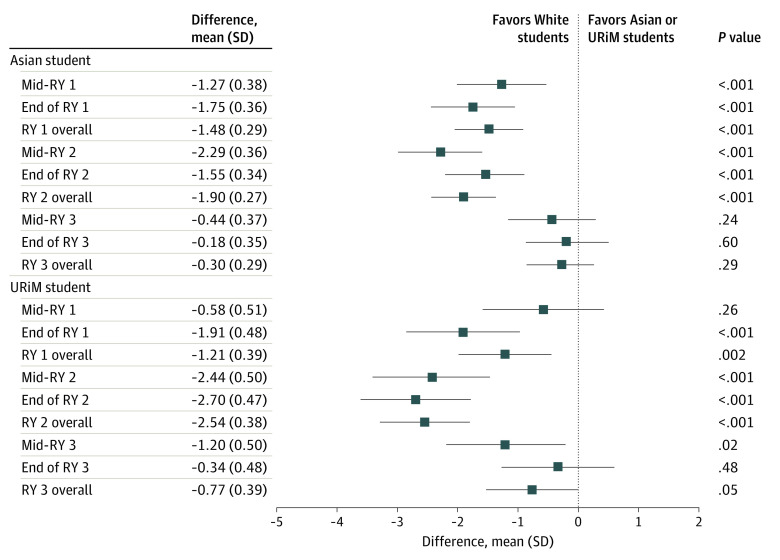
The primary outcome was midyear and year-end total ACGME Milestone scores for underrepresented in medicine (URiM [Hispanic only; non-Hispanic American Indian, Alaska Native, or Native Hawaiian/Pacific Islander only; or non-Hispanic Black/African American]) and Asian residents compared with White residents as determined by their Clinical Competency Committees and residency program directors. Differences in scores between Asian and URiM residents compared with White residents were also compared for each of the 6 competency domains as supportive outcomes.
The study cohort included 9026 residents from 305 internal medicine residency programs. Of these residents, 3994 (44.2%) were female, 3258 (36.1%) were Asian, 1216 (13.5%) were URiM, and 4552 (50.4%) were White. In the fully adjusted model, no difference was found in the initial midyear total Milestone scores between URiM and White residents, but there was a difference between Asian and White residents, which favored White residents (mean [SD] difference in scores for Asian residents: -1.27 [0.38]; P < .001). In the second year of training, White residents received increasingly higher scores relative to URiM and Asian residents. These racial disparities peaked in postgraduate year (PGY) 2 (mean [SD] difference in scores for URiM residents, -2.54 [0.38]; P < .001; mean [SD] difference in scores for Asian residents, -1.9 [0.27]; P < .001). By the final year 3 assessment, the gap between White and Asian and URiM residents' scores narrowed, and no racial or ethnic differences were found. Trends in racial and ethnic differences among the 6 competency domains mirrored total Milestone scores, with differences peaking in PGY2 and then decreasing in PGY3 such that parity in assessment was reached in all competency domains by the end of training.
In this cohort study, URiM and Asian internal medicine residents received lower ratings on performance assessments than their White peers during the first and second years of training, which may reflect racial bias in assessment. This disparity in assessment may limit opportunities for physicians from minoritized racial and ethnic groups and hinder physician workforce diversity.
先前的研究表明,在学术医疗中心,医学生评估、奖项和教师晋升方面存在种族和民族不平等现象。关于研究生医学教育层面类似的种族和民族差异的数据很少。
研究全国内科住院医师队列中种族和民族与表现评估之间的关系。
设计、设置和参与者:这项回顾性队列研究评估了美国经住院医师教育认证委员会(ACGME)认证的内科住院医师项目 2016 年和 2017 年毕业班级中 9026 名内科住院医师的表现评估。分析于 2020 年 7 月 1 日至 2022 年 6 月 31 日进行。
主要结局是由临床能力委员会和住院医师项目主任确定的,医学领域代表性不足的(URiM [仅西班牙裔;非西班牙裔美洲印第安人、阿拉斯加原住民或夏威夷原住民/太平洋岛民;或非西班牙裔黑人/非裔美国人])和亚洲住院医师与白人住院医师相比,在中期和年末的 ACGME 里程碑总评分。作为支持性结果,还比较了每个 6 个能力领域中,亚洲和 URiM 住院医师与白人住院医师之间的评分差异。
研究队列包括来自 305 个内科住院医师项目的 9026 名住院医师。其中,3994 名(44.2%)为女性,3258 名(36.1%)为亚洲人,1216 名(13.5%)为 URiM,4552 名(50.4%)为白人。在完全调整的模型中,URiM 和白人住院医师之间的初始中期总里程碑评分没有差异,但亚洲和白人住院医师之间存在差异,这有利于白人住院医师(亚洲住院医师的评分差异为-1.27 [0.38];P<0.001)。在培训的第二年,白人住院医师的评分相对于 URiM 和亚洲住院医师的评分逐渐提高。这些种族差异在住院医师培训的第 2 年(URiM 住院医师的评分差异,-2.54 [0.38];P<0.001;亚洲住院医师的评分差异,-1.9 [0.27];P<0.001)达到顶峰。到第 3 年的最终评估时,白人住院医师和亚洲住院医师以及 URiM 住院医师的评分差距缩小,且在所有能力领域中都没有发现种族或民族差异。在 6 个能力领域中种族和民族差异的趋势与总里程碑评分相似,在第 2 年住院医师培训期间达到峰值,然后在第 3 年住院医师培训期间下降,从而在培训结束时达到所有能力领域的评估平等。
在这项队列研究中,URiM 和亚洲内科住院医师在培训的第一和第二年的表现评估中得分低于白人同龄人,这可能反映了评估中的种族偏见。这种评估上的差异可能会限制少数族裔和种族群体医生的机会,并阻碍医生劳动力的多样性。