Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China.
Department of Epidemiology, Centre for Global Cardio-Metabolic Health, Brown University, Providence, RI, United States.
Front Endocrinol (Lausanne). 2022 Dec 15;13:1012383. doi: 10.3389/fendo.2022.1012383. eCollection 2022.
The relationship between the total cholesterol/high-density lipoprotein cholesterol (TC/HDL-C) ratio and all-cause and cardiovascular mortality has not been elucidated. Herein, we intend to probe the effect of the TC/HDL-C ratio on all-cause and cardiovascular mortality in the general population.
From the 1999-2014 National Health and Nutrition Examination Surveys (NHANES), a total of 32,405 health participants aged ≥18 years were included. The TC/HDL-C levels were divided into five groups: Q1: <2.86, Q2: 2.86-3.46, Q3: 3.46-4.12, Q4: 4.12-5.07, Q5: >5.07. Multivariate Cox regression models were used to explore the relationship between the TC/HDL-C ratio and cardiovascular and all-cause mortality. Two-piecewise linear regression models and restricted cubic spline regression were used to explore nonlinear and irregularly shaped relationships. Kaplan-Meier survival curve and subgroup analyses were conducted.
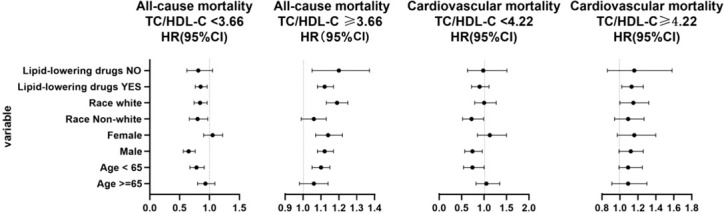
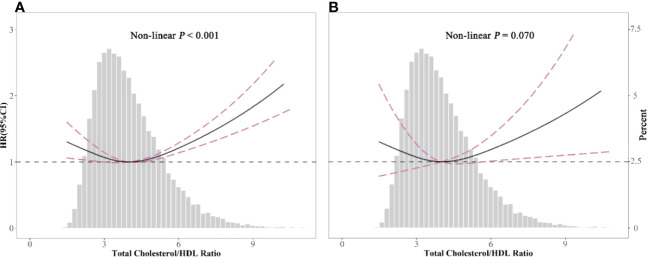
The population comprised 15,675 men and 16,730 women with a mean age of 43 years. During a median follow-up of 98 months (8.1 years), 2,859 mortality cases were recorded. The TC/HDL-C ratio and all-cause mortality showed a nonlinear association after adjusting for confounding variables in the restricted cubic spline analysis. Hazard ratios (HRs) of all-cause mortality were particularly positively related to the level of TC/HDL-C ratio in the higher range >5.07 and in the lower range <2.86 (HR 1.26; 95% CI 1.10, 1.45; HR 1.18; 95% CI 1.00, 1.38, respectively), although the HRs of cardiovascular disease mortality showed no difference among the five groups. In the two-piecewise linear regression model, a TC/HDL-C ratio range of ≥4.22 was positively correlated with cardiovascular mortality (HR 1.13; 95% CI 1.02, 1.25). In the subgroup analysis, a nonlinear association between TC/HDL-C and all-cause mortality was found in those aged <65 years, men, and the no lipid drug treatment population.
A nonlinear association between the TC/HDL-C ratio and all-cause mortality was found, indicating that a too-low or too-high TC/HDL-C ratio might increase all-cause mortality. However, for cardiovascular mortality, it does not seem so. The cutoff value was 4.22. The individuals had higher cardiovascular mortality with a TC/HDL-C ratio >4.22.
总胆固醇/高密度脂蛋白胆固醇(TC/HDL-C)比值与全因和心血管死亡率之间的关系尚未阐明。本研究旨在探讨 TC/HDL-C 比值对一般人群全因和心血管死亡率的影响。
本研究纳入了 1999 年至 2014 年全国健康与营养调查(NHANES)中年龄≥18 岁的 32405 名健康参与者。TC/HDL-C 水平分为五组:Q1:<2.86,Q2:2.86-3.46,Q3:3.46-4.12,Q4:4.12-5.07,Q5:>5.07。采用多变量 Cox 回归模型探讨 TC/HDL-C 比值与心血管和全因死亡率之间的关系。采用两段线性回归模型和限制性三次样条回归模型探讨非线性和非规则形状的关系。进行 Kaplan-Meier 生存曲线和亚组分析。
该人群包括 15675 名男性和 16730 名女性,平均年龄为 43 岁。在中位随访 98 个月(8.1 年)期间,记录了 2859 例死亡事件。经协变量调整后的限制性立方样条分析显示,TC/HDL-C 比值与全因死亡率呈非线性关联。全因死亡率的危险比(HRs)与 TC/HDL-C 比值较高范围(>5.07)和较低范围(<2.86)呈正相关(HR 1.26;95%CI 1.10,1.45;HR 1.18;95%CI 1.00,1.38,分别),尽管心血管疾病死亡率的 HRs 在五组之间无差异。在两段线性回归模型中,TC/HDL-C 比值范围≥4.22 与心血管死亡率呈正相关(HR 1.13;95%CI 1.02,1.25)。在亚组分析中,TC/HDL-C 与全因死亡率之间存在非线性关联,在年龄<65 岁、男性和未使用降脂药物的人群中更为明显。
TC/HDL-C 比值与全因死亡率之间呈非线性关联,提示 TC/HDL-C 比值过低或过高可能会增加全因死亡率。然而,对于心血管死亡率来说,情况似乎并非如此。当 TC/HDL-C 比值>4.22 时,心血管死亡率更高。