Department of Medical Physics, Pamela Youde Nethersole Eastern Hospital, Hong Kong, China.
Department of Clinical Oncology, Pamela Youde Nethersole Eastern Hospital, Hong Kong, China.
Radiat Oncol. 2023 Jan 11;18(1):9. doi: 10.1186/s13014-022-02195-z.
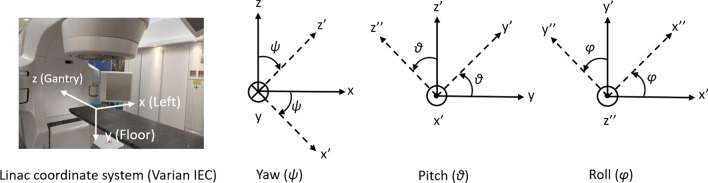
To investigate the geometric and dosimetric impacts of intra-fractional movement for patients with single or multiple brain metastasis treated using Varian Hyperarc™ mono-isocentric radiosurgery.
A total of 50 single or hypo-fractionated Hyperarc™ treatment courses (118 lesions) were included in the analysis. Intra-fractional translational and rotational movements were quantified according to the post-treatment cone-beam CT (CBCT). Geometric displacements of all targets were calculated individually based on the assessed head movement in each treatment fraction and their relationships with treatment time and target-to-isocenter distances were studied. For dosimetric analysis, only single-fraction treatments (56 lesions) were included. Re-planning was performed with 0, 1, and 2 mm planning target volume (PTV) margins. Doses were then re-calculated on rotated CT images with isocenter shifted which emulate the change in patient treatment position. Target coverage, target and normal brain doses before and after intra-fractional movement were compared.
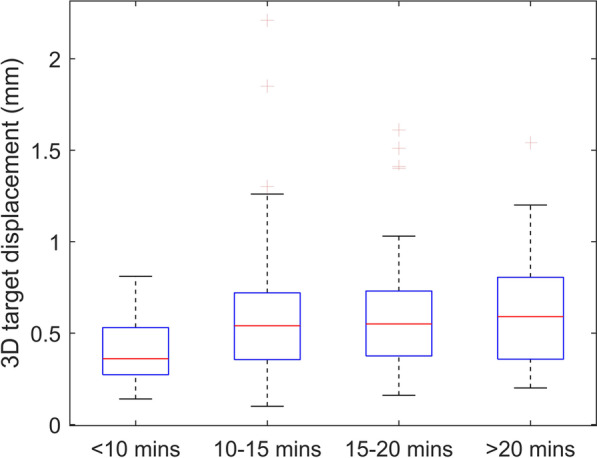
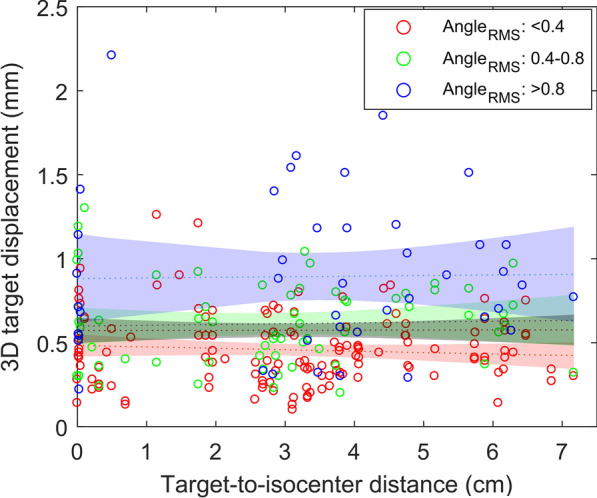
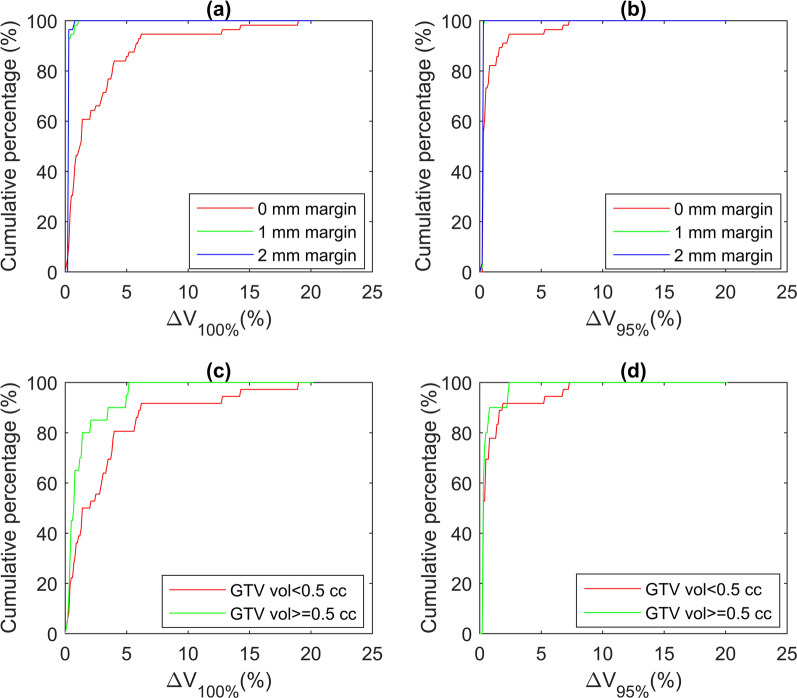
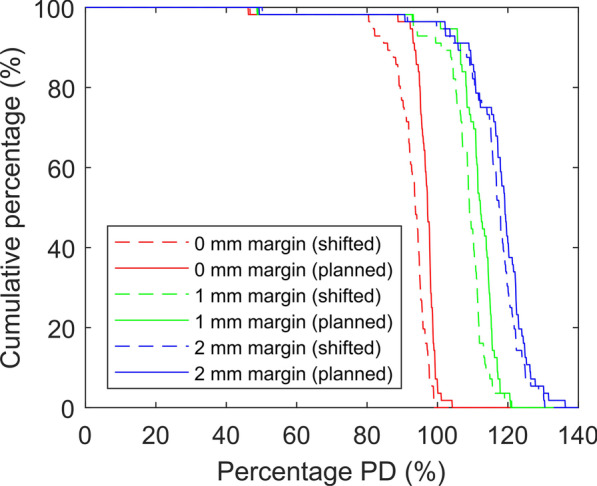
The mean 3D target displacements was 0.6 ± 0.3 (SD) mm. Target shifts for patients treated within 10 min were significantly smaller than those treated in longer sessions. No correlation was found between target shift and target-to-isocenter distance as the origin of head rotation was not located at the isocenter. Loss of target coverage and minimum Gross Tumor Volume (GTV) dose due to intra-fractional movement were apparent only when no margin was used, leading to an extra 23% of the targets violating the dose acceptance criteria, in contrast, the effects on normal brain V were negligible regardless of the margin used. The use of 1 mm PTV margin can compensate clinically significant geographical miss caused by intra-fractional movements while limiting V to within dose criteria for 88% of the cases. The plan acceptance rate (fulfillment of both target and normal brain dose criteria) after intra-fractional movement was also the highest with the 1 mm margin.
Although intra-fractional movements during Hyperarc™ treatments were small, there were substantial dosimetric effects due to the sharp dose fall-off near target boundaries. These effects could be mitigated by using a 1 mm PTV margin and maintaining the effective treatment time to within 10 min.
研究使用瓦里安 Hyperarc™单等中心放射外科治疗单个或多个脑转移瘤患者的分次内运动的几何和剂量学影响。
本研究共纳入 50 例单或亚分次 Hyperarc™治疗疗程(118 个病灶)。根据治疗后锥形束 CT(CBCT)评估,量化分次内的平移和旋转运动。根据每个治疗分次中评估的头部运动,单独计算所有靶区的几何位移,并研究其与治疗时间和靶区到等中心距离的关系。对于剂量学分析,仅纳入单次分割治疗(56 个病灶)。使用 0、1 和 2 毫米计划靶区(PTV)边界进行重新计划。然后在等中心移位的旋转 CT 图像上重新计算剂量,以模拟患者治疗位置的变化。比较分次内运动前后靶区覆盖、靶区和正常脑组织剂量。
平均 3D 靶区位移为 0.6±0.3(SD)毫米。治疗时间在 10 分钟以内的患者的靶区移位明显小于治疗时间较长的患者。未发现靶区移位与靶区到等中心距离之间存在相关性,因为头部旋转的原点不在等中心。仅当未使用边界时,由于分次内运动导致的靶区覆盖率和最小总肿瘤体积(GTV)剂量损失才明显,导致 23%的靶区违反剂量接受标准,相比之下,无论使用何种边界,对正常脑组织 V 的影响都可以忽略不计。使用 1 毫米 PTV 边界可以补偿由于分次内运动导致的临床显著地理缺失,同时将 88%的病例的 V 限制在剂量标准内。使用 1 毫米 PTV 边界时,分次内运动后的计划接受率(同时满足靶区和正常脑组织剂量标准)也是最高的。
尽管 Hyperarc™治疗期间的分次内运动较小,但由于靶区边界附近的剂量急剧下降,仍存在显著的剂量学影响。通过使用 1 毫米 PTV 边界并将有效治疗时间保持在 10 分钟以内,可以减轻这些影响。