Kang Min-Gu, Choi Jung-Yeon, Yoo Hyun-Jung, Park Si-Young, Kim Yoonhee, Kim Ji Yoon, Kim Sun-Wook, Kim Cheol-Ho, Kim Kwang-Il
Department of Internal Medicine, Chonnam National University Bitgoeul Hospital, Gwangju, Republic of Korea.
Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam-si, Republic of Korea.
Front Nutr. 2023 Jan 5;9:1046985. doi: 10.3389/fnut.2022.1046985. eCollection 2022.
Malnutrition is prevalent among hospitalized older patients. Therefore, this study aimed to investigate the association between nutritional status [assessed using the Mini Nutritional Assessment (MNA) and serum albumin levels] and adverse outcomes in hospitalized older patients. We also aimed to compare the predictive utility of our findings.
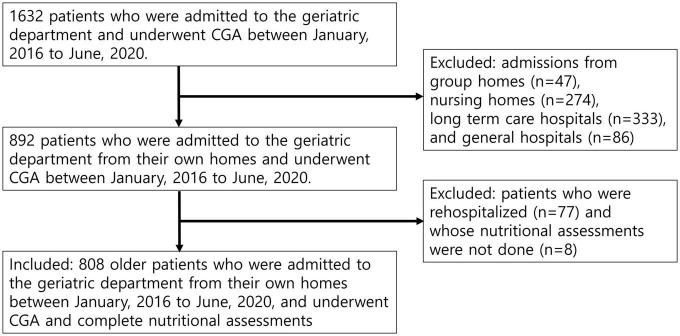
This retrospective cohort study was conducted between January 2016 and June 2020. In total, 808 older patients (aged ≥ 65 years, mean age 82.8 ± 6.70 years, 45.9% male) admitted to the acute geriatric unit were included in our sample. Comprehensive geriatric assessments, including the MNA, were performed. Malnutrition and risk of malnutrition were defined as MNA < 17, albumin < 3.5 g/dL and 17 ≤ MNA ≤ 24, 3.5 g/dL ≤ albumin < 3.9 g/dL, respectively. The primary outcome was that patients could not be discharged to their own homes. The secondary outcomes were overall all-cause mortality, 3-month all-cause mortality, and incidence of geriatric syndrome, including delirium, falls, and newly developed or worsening pressure sores during hospitalization.
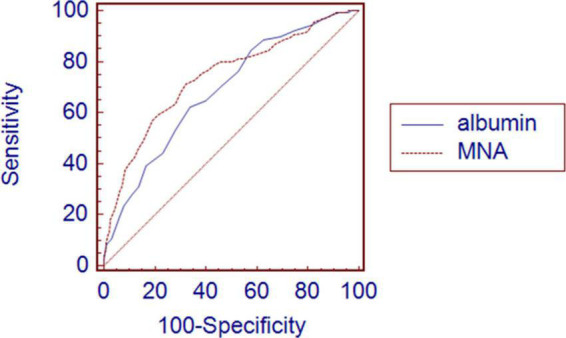
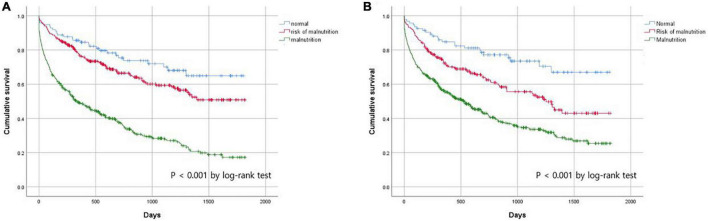
Poor nutritional status was associated with older age; female sex; admission from the emergency room; high risk of pressure sores and falls; lower physical and cognitive function; higher depressive score; and lower serum albumin, protein, cholesterol, and hemoglobin levels. In the fully adjusted model, malnutrition assessed using the MNA predicted discharge to nursing homes or long-term care hospitals [odds ratio (OR) 5.822, 95% confidence interval (CI): 2.092-16.199, = 0.001], geriatric syndrome (OR 2.069, 95% CI: 1.007-4.249, = 0.048), and 3-month mortality (OR 3.519, 95% CI: 1.254-9.872, = 0.017). However, malnutrition assessed using albumin levels could only predict 3-month mortality (OR 3.848, 95% CI: 1.465-10.105, = 0.006). The MNA predicted 3-month mortality with higher precision than serum albumin levels ( = 0.034) when comparing the areas under the receiver operating characteristic curve.
Nutritional risk measured by the MNA was an independent predictor of various negative outcomes in hospitalized older patients. Poor nutritional status assessed by serum albumin levels, the most widely used biochemical marker, could predict mortality, but not the development of geriatric syndrome or discharge location reflecting functional status.
营养不良在住院老年患者中普遍存在。因此,本研究旨在调查营养状况[采用微型营养评定法(MNA)和血清白蛋白水平进行评估]与住院老年患者不良结局之间的关联。我们还旨在比较我们研究结果的预测效用。
本回顾性队列研究于2016年1月至2020年6月进行。我们纳入了808例入住急性老年病科的老年患者(年龄≥65岁,平均年龄82.8±6.70岁,男性占45.9%)。进行了包括MNA在内的综合老年评估。营养不良和营养不良风险分别定义为MNA<17、白蛋白<3.5 g/dL以及17≤MNA≤24、3.5 g/dL≤白蛋白<3.9 g/dL。主要结局是患者无法出院回家。次要结局包括总体全因死亡率、3个月全因死亡率以及老年综合征的发生率,老年综合征包括谵妄、跌倒以及住院期间新出现或加重的压疮。
营养状况不佳与年龄较大、女性、从急诊室入院、压疮和跌倒风险较高、身体和认知功能较低、抑郁评分较高以及血清白蛋白、蛋白质、胆固醇和血红蛋白水平较低有关。在完全调整模型中,使用MNA评估的营养不良可预测入住养老院或长期护理医院(比值比[OR]5.822,95%置信区间[CI]:2.092 - 16.199,P = 0.001)、老年综合征(OR 2.069,95%CI:1.007 - 4.249,P = 0.048)以及3个月死亡率(OR 3.519,95%CI:1.254 - 9.872,P = 0.017)。然而,使用白蛋白水平评估的营养不良仅能预测3个月死亡率(OR 3.848,95%CI:1.465 - 10.105,P = 0.006)。在比较受试者工作特征曲线下面积时,MNA预测3个月死亡率的精度高于血清白蛋白水平(P = 0.034)。
MNA测量的营养风险是住院老年患者各种负面结局的独立预测因素。血清白蛋白水平是最广泛使用的生化标志物,通过其评估的营养状况不佳可预测死亡率,但不能预测老年综合征的发生或反映功能状态的出院地点。