Department of Cardiology Keio University School of Medicine Tokyo Japan.
Department of Healthcare Quality Assessment The University of Tokyo Tokyo Japan.
J Am Heart Assoc. 2023 Feb 7;12(3):e027689. doi: 10.1161/JAHA.122.027689. Epub 2023 Jan 25.
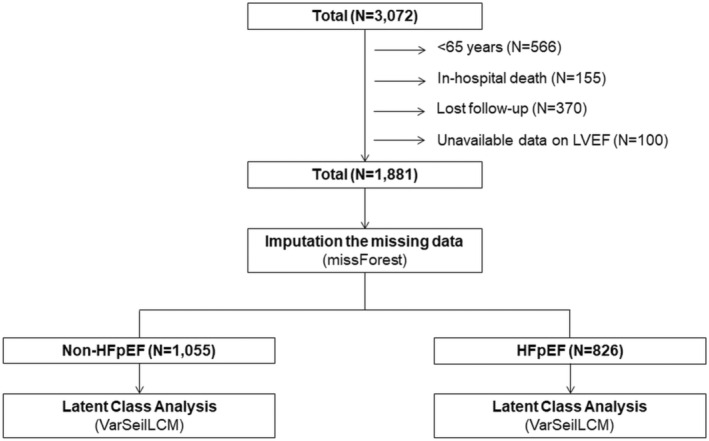
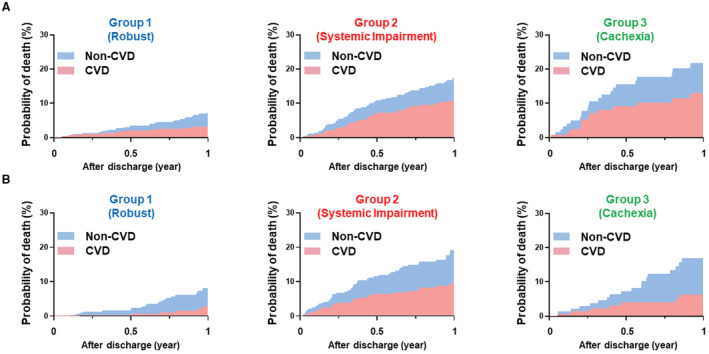
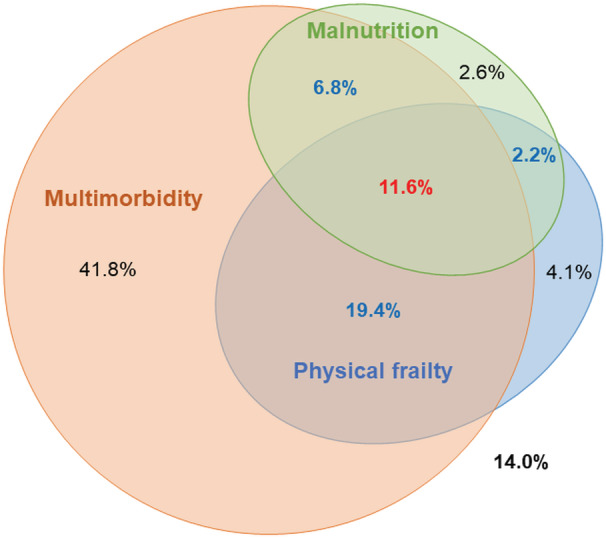
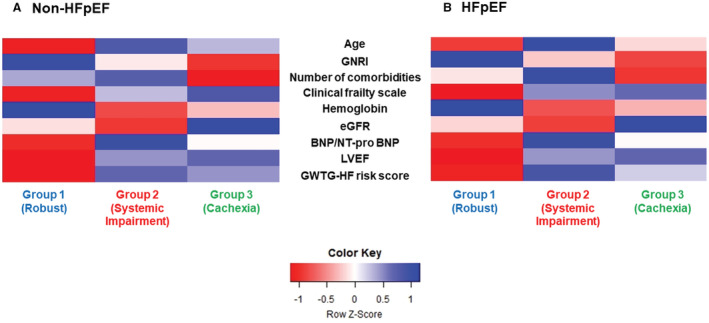
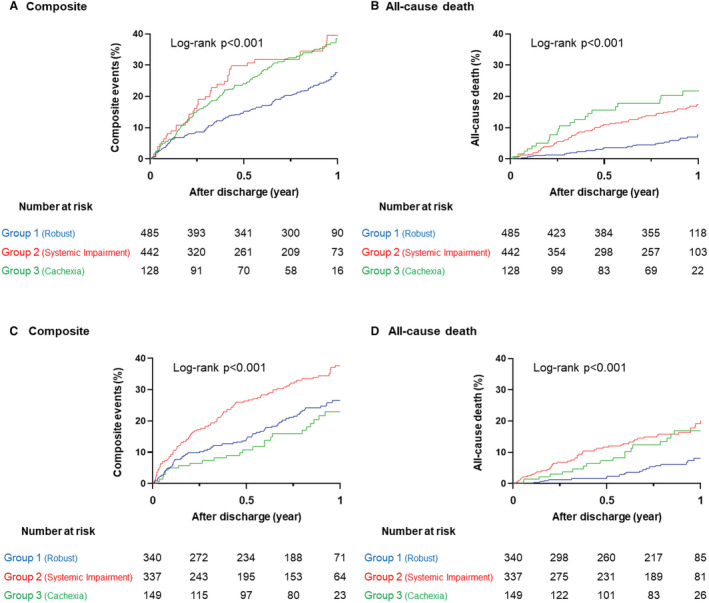
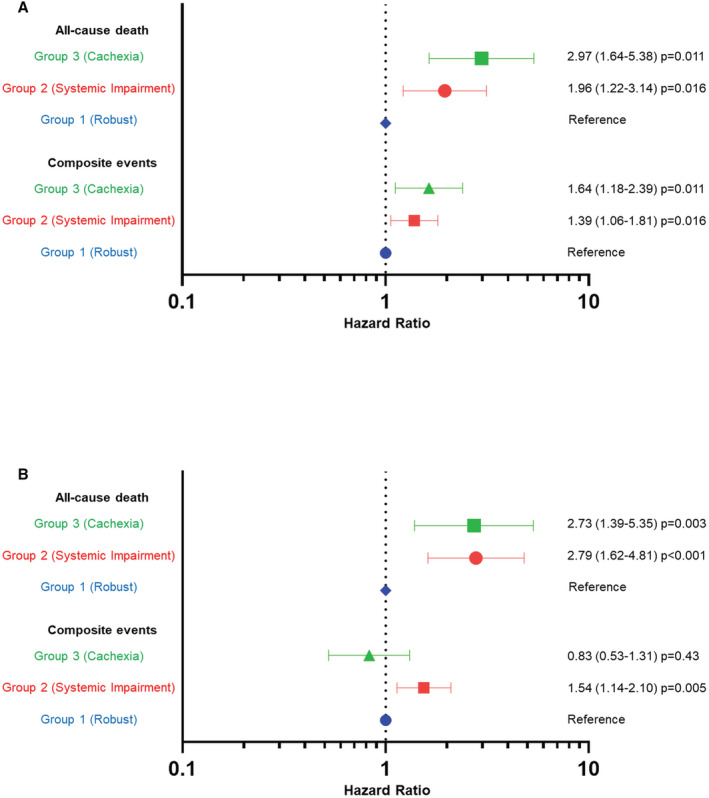
Background The burden of noncardiovascular conditions is becoming increasingly prevalent in patients with heart failure (HF). We aimed to identify novel phenogroups incorporating noncardiovascular conditions to facilitate understanding and risk stratification in elderly patients with HF. Methods and Results Data from a total of 1881 (61.2%) patients aged ≥65 years were extracted from a prospective multicenter registry of patients hospitalized for acute HF (N=3072). We constructed subgroups of patients with HF with preserved ejection fraction (HFpEF; N=826, 43.9%) and those with non-HFpEF (N=1055, 56.1%). Latent class analysis was performed in each subgroup using 17 variables focused on noncardiovascular conditions (including comorbidities, Clinical Frailty Scale, and Geriatric Nutritional Risk Index). The latent class analysis revealed 3 distinct clinical phenogroups in both HFpEF and non-HFpEF subgroups: (1) robust physical and nutritional status (Group 1: HFpEF, 41.2%; non-HFpEF, 46.0%); (2) multimorbid patients with renal impairment (Group 2: HFpEF, 40.8%; non-HFpEF, 41.9%); and (3) malnourished patients (Group 3: HFpEF, 18.0%; non-HFpEF, 12.1%). After multivariable adjustment, compared with Group 1, patients in Groups 2 and 3 had a higher risk for all-cause death over the 1-year postdischarge period (hazard ratio [HR], 2.79 [95% CI, 1.64-4.81] and HR, 2.73 [95% CI, 1.39-5.35] in HFpEF; HR, 1.96 [95% CI, 1.22-3.14] and HR, 2.97 [95% CI, 1.64-5.38] in non-HFpEF; respectively). Conclusions In elderly patients with HF, the phenomapping focused on incorporating noncardiovascular conditions identified 3 phenogroups, each representing distinct clinical outcomes, and the discrimination pattern was similar for both patients with HFpEF and non-HFpEF. This classification provides novel risk stratification and may aid in clinical decision making.
非心血管疾病的负担在心力衰竭(HF)患者中越来越普遍。我们旨在确定包含非心血管疾病的新表型组,以方便理解和对老年 HF 患者进行风险分层。
从一项前瞻性多中心急性 HF 住院患者登记研究中提取了共 1881 名(61.2%)≥65 岁患者的数据(N=3072)。我们构建了射血分数保留的 HF(HFpEF;N=826,43.9%)和非 HFpEF(N=1055,56.1%)患者的亚组。使用 17 个侧重于非心血管疾病的变量(包括合并症、临床虚弱量表和老年营养风险指数),在每个亚组中进行潜在类别分析。潜在类别分析在 HFpEF 和非 HFpEF 亚组中均显示出 3 个不同的临床表型组:(1)身体和营养状况良好(第 1 组:HFpEF,41.2%;非 HFpEF,46.0%);(2)伴有肾功能损害的多合并症患者(第 2 组:HFpEF,40.8%;非 HFpEF,41.9%);和(3)营养不良的患者(第 3 组:HFpEF,18.0%;非 HFpEF,12.1%)。多变量调整后,与第 1 组相比,第 2 组和第 3 组患者在出院后 1 年内全因死亡风险更高(HFpEF 中的危险比[HR],2.79[95%可信区间,1.64-4.81]和 HR,2.73[95%可信区间,1.39-5.35];非 HFpEF 中的 HR,1.96[95%可信区间,1.22-3.14]和 HR,2.97[95%可信区间,1.64-5.38])。
在老年 HF 患者中,侧重于纳入非心血管疾病的表型映射确定了 3 个表型组,每个组代表不同的临床结局,并且这种区分模式在 HFpEF 和非 HFpEF 患者中相似。这种分类提供了新的风险分层,并可能有助于临床决策。