Obstetrics and Gynecology Hospital, Fudan University, Shanghai, China.
J Ovarian Res. 2023 Jan 30;16(1):28. doi: 10.1186/s13048-023-01102-8.
To compare the prognosis of lymphatic metastasis in type I and type II epithelial ovarian cancer (OC) and to identify the risk factors for pelvic lymph node metastases (PLNs) and para-aortic lymph node metastases (PALNs).
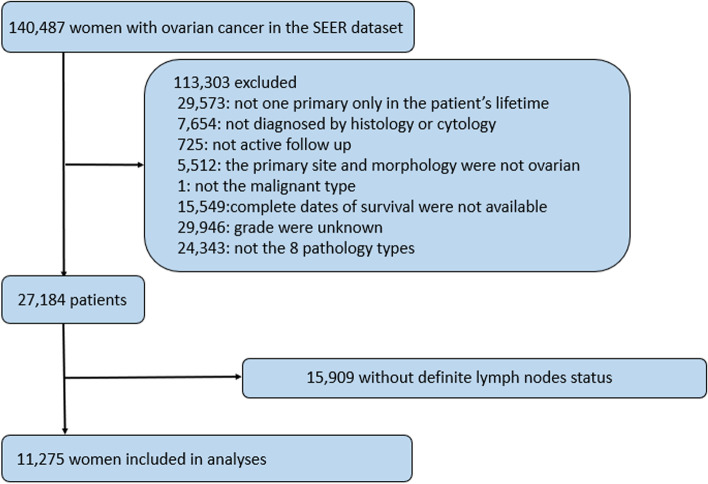
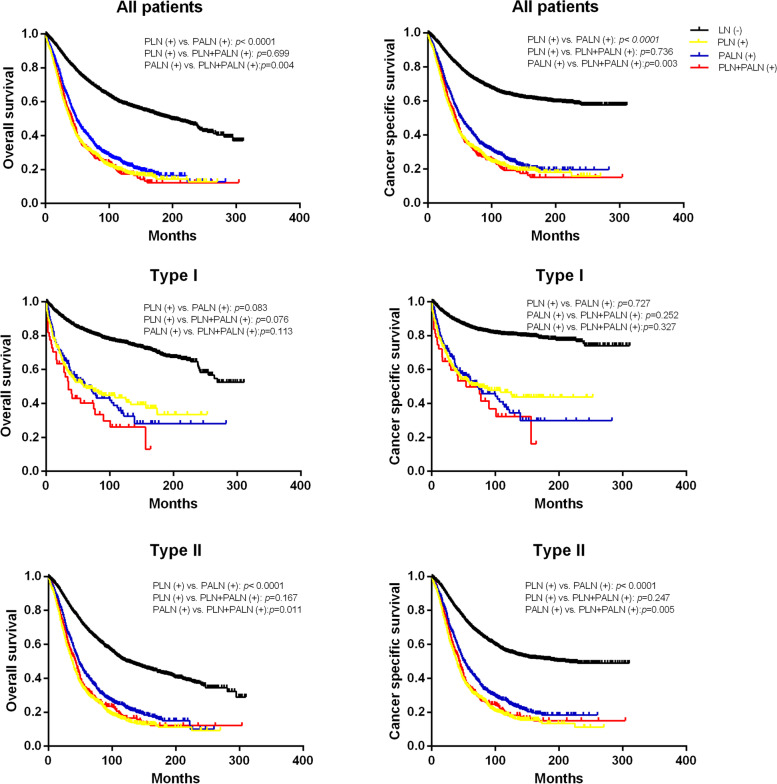
Patients diagnosed with epithelial OC were collected from the Surveillance, Epidemiology, and End Results (SEER) database. Overall survival (OS) and cancer-specific survival (CSS) were estimated. The Cox proportional hazards regression model was used to identify independent predictors of survival.
A total of 11,275 patients with OC were enrolled, including 31.2% with type I and 68.8% with type II. Type II and high tumour stage were risk factors for lymph node involvement (p < 0.05). The overall rate of lymph node metastasis in type I was 11.8%, and that in type II was 36.7%. In the type I group, the lymph node metastasis rates in stages T1, T2, T3 and TM were 3.2%, 14.5%, 40.4% and 50.0%, respectively. In the type II group, these rates were 6.4%, 20.4%, 54.1% and 61.1%, respectively. Age and tumour size had little effect on lymph node metastasis, and grade 3 was not always a risk factor. For the type I group, the 10-year CSS rates of LN(-), PLN( +), PALN( +), and PLN + PALN( +) were 80.6%, 46.6%, 36.3%, and 32.3%, respectively. The prognosis of PLN ( +) was better than that of PALN ( +) in the type I group (p > 0.05). For the type II group, the 10-year CSS rates of LN(-), PLN( +), PALN( +), and PLN + PALN( +) were 55.6%, 18.5%, 25.7%, and 18.2%, respectively. PALN ( +) had a significantly better prognosis than PLN ( +) in the type II group (p < 0.05).
The clinical characteristics and prognoses of patients with type I and type II OC differed greatly. Patients with type II and higher tumour stages had poorer prognoses. Type I with PALN metastasis and type II with PLN metastasis indicated a worse prognosis. Patients with stage TI did not require lymph node dissection, especially in the type I group.
比较 I 型和 II 型上皮性卵巢癌(OC)的淋巴转移预后,并确定盆腔淋巴结转移(PLN)和腹主动脉旁淋巴结转移(PALN)的风险因素。
从监测、流行病学和最终结果(SEER)数据库中收集上皮性 OC 患者。估计总生存率(OS)和癌症特异性生存率(CSS)。使用 Cox 比例风险回归模型确定生存的独立预测因素。
共纳入 11275 例 OC 患者,其中 31.2%为 I 型,68.8%为 II 型。II 型和高肿瘤分期是淋巴结受累的危险因素(p<0.05)。I 型的总体淋巴结转移率为 11.8%,II 型为 36.7%。在 I 型组中,T1、T2、T3 和 TM 期的淋巴结转移率分别为 3.2%、14.5%、40.4%和 50.0%。在 II 型组中,这些比率分别为 6.4%、20.4%、54.1%和 61.1%。年龄和肿瘤大小对淋巴结转移影响不大,3 级并不总是危险因素。对于 I 型组,LN(-)、PLN(+)、PALN(+)和 PLN+PALN(+)的 10 年 CSS 率分别为 80.6%、46.6%、36.3%和 32.3%。I 型组 PLN(+)的预后优于 PALN(+)(p>0.05)。对于 II 型组,LN(-)、PLN(+)、PALN(+)和 PLN+PALN(+)的 10 年 CSS 率分别为 55.6%、18.5%、25.7%和 18.2%。II 型组 PALN(+)的预后明显优于 PLN(+)(p<0.05)。
I 型和 II 型 OC 患者的临床特征和预后差异很大。II 型和较高肿瘤分期的患者预后较差。I 型伴 PALN 转移和 II 型伴 PLN 转移提示预后较差。T1 期患者无需进行淋巴结清扫,尤其是 I 型患者。