Department of Medicine, Massachusetts General Hospital, Boston, MA, USA.
Department of Hematology Oncology, Dana-Farber Cancer Institute, Boston, MA, USA.
Oncologist. 2023 Mar 17;28(3):252-257. doi: 10.1093/oncolo/oyac275.
Iniparib (BSI-201), a novel anticancer agent thought to have poly(ADP-ribose) polymerase (PARP) inhibitory activity and synergy with both gemcitabine and carboplatin (GC) was evaluated in 2 cohorts with GC.
Parallel multicenter, single-arm, phase II studies using a Simon two-stage design. Eligible patients had a histological diagnosis of epithelial ovarian carcinoma, fallopian tube cancer, or primary peritoneal carcinoma and demonstration of platinum-sensitive (≥6 months [mo]) or -resistant disease (relapse 2-6 mo post-platinum). Carboplatin (AUC 4 IV day 1), gemcitabine (1000 mg/m2 IV days 1 and 8), and iniparib (5.6 mg/kg IV days 1, 4, 8, and 11) were given on a 21-day cycle.
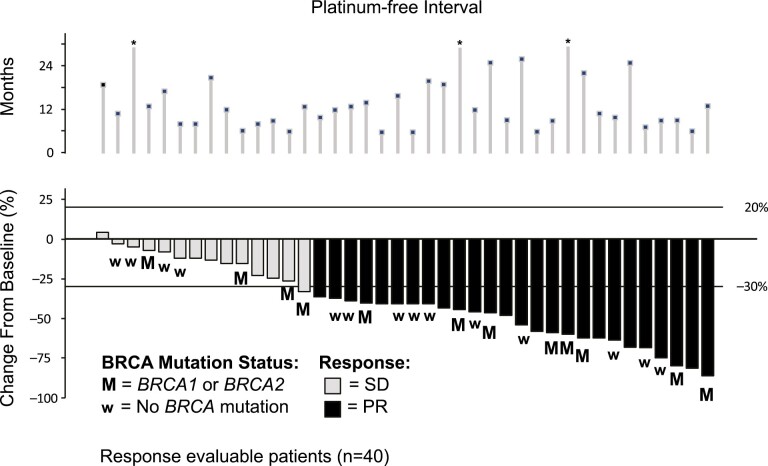
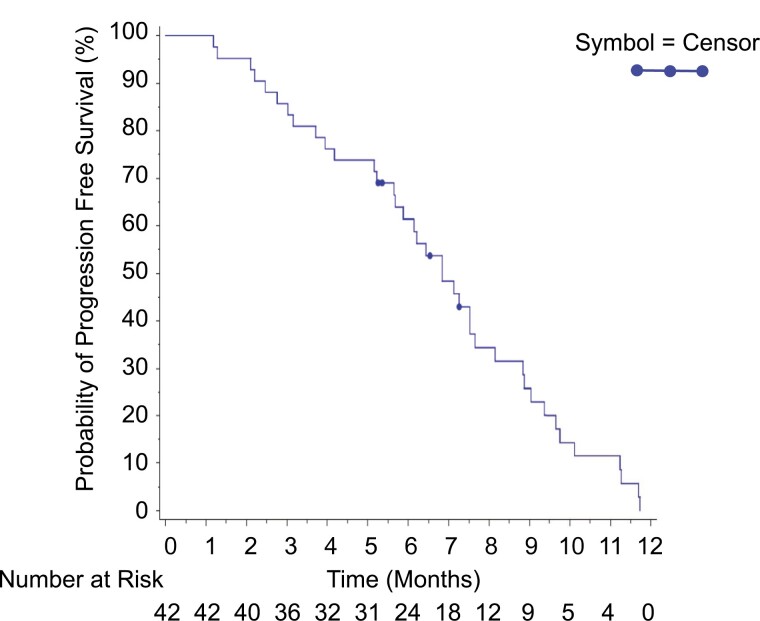
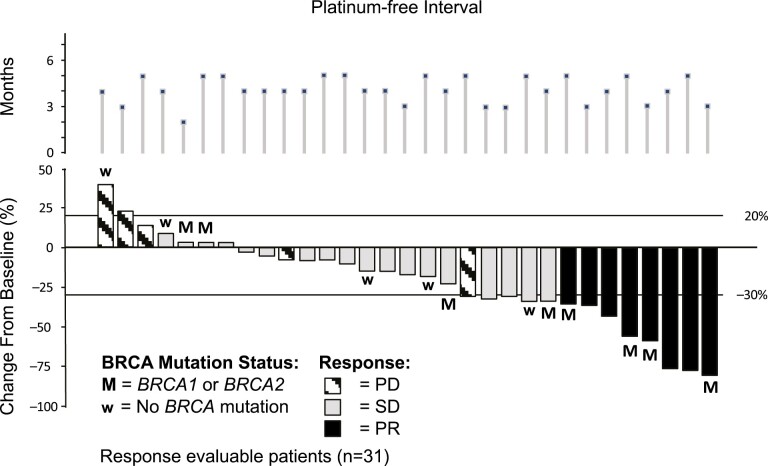
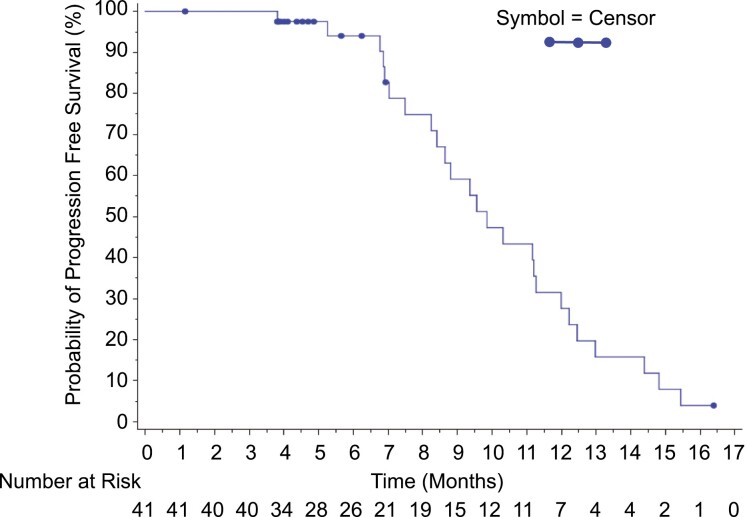
The overall response rate (ORR RECIST 1.0) in platinum sensitive disease was 66% (95% CI, 49-80) with a higher response rate in the 15 pts with germline BRCA mutations (gBRCAmut) (73%). Median PFS was 9.9 (95% CI, 8.2-11.3) months. In the platinum resistant population the ORR was 26% (95% CI, 14-42), however in the 11 pts for whom BRCA mutation was present, the best overall response was PR in 5 (46%). Median PFS was 6.8 months (range, 5.7-7.7 months). Notably, among the 17 CA-125-response-evaluable patients who did not achieve tumor response, 7 (41.2%) patients had a CA125 response, and 93% has clinical benefit (CR + PR + SD). The GCI combination was generally well tolerated despite a high incidence of thrombocytopenia and neutropenia, with no new toxicities.
Given the subsequent lack of efficacy demonstrated for iniparib in breast cancer, these are studies of GC and demonstrate a higher than traditionally appreciated activity in patients with platinum-sensitive and -resistant recurrent ovarian cancer, especially in patients that harbor a BRCA mutation, resetting the benchmark for efficacy in phase II trials. (ClinicalTrials.gov Identifiers: NCT01033292 & NCT01033123).
Iniparib(BSI-201)是一种新型抗癌药物,具有聚(ADP-核糖)聚合酶(PARP)抑制活性,并与吉西他滨和卡铂(GC)具有协同作用,在 2 个 GC 队列中进行了评估。
采用 Simon 两阶段设计的平行多中心、单臂、二期研究。合格患者的组织学诊断为上皮性卵巢癌、输卵管癌或原发性腹膜癌,并证明对铂类敏感(≥6 个月[mo])或耐药(复发后 2-6 mo 铂类)。卡铂(AUC 4 IV 天 1 次)、吉西他滨(1000 mg/m2 IV 天 1 次和 8 次)和 iniparib(5.6 mg/kg IV 天 1 次、4 次、8 次和 11 次)在 21 天周期内给予。
铂类敏感疾病的总体缓解率(RECIST 1.0 的 ORR)为 66%(95%CI,49-80),在 15 名种系 BRCA 突变(gBRCAmut)患者中(73%)的反应率更高。中位无进展生存期(PFS)为 9.9 个月(95%CI,8.2-11.3)。在铂类耐药人群中,ORR 为 26%(95%CI,14-42),然而,在 11 名存在 BRCA 突变的患者中,最佳总体反应为 PR 占 5 例(46%)。中位 PFS 为 6.8 个月(范围,5.7-7.7 个月)。值得注意的是,在 17 名可评估 CA-125 反应的患者中,有 7 名(41.2%)患者有 CA125 反应,93%的患者有临床获益(CR+PR+SD)。尽管血小板减少症和中性粒细胞减少症的发生率很高,但 GCI 联合治疗总体上耐受性良好,无新的毒性作用。
鉴于随后在乳腺癌中缺乏 iniparib 的疗效,这些是 GC 的研究,并在铂类敏感和耐药复发性卵巢癌患者中显示出高于传统的活性,尤其是在携带 BRCA 突变的患者中,为 II 期试验中的疗效设定了新的基准。(ClinicalTrials.gov 标识符:NCT01033292 & NCT01033123)。