Department of Hygiene and Public Health, Teikyo University School of Medicine, Tokyo, Japan.
Research Unit Hypertension and Cardiovascular Epidemiology, KU Leuven Department of Cardiovascular Sciences, University of Leuven, Leuven, Belgium.
Hypertens Res. 2023 Apr;46(4):934-949. doi: 10.1038/s41440-023-01191-4. Epub 2023 Feb 3.
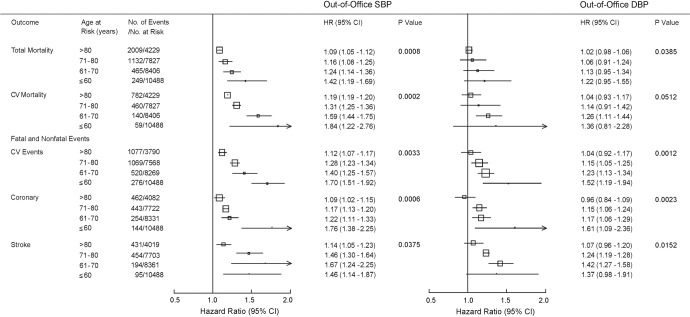
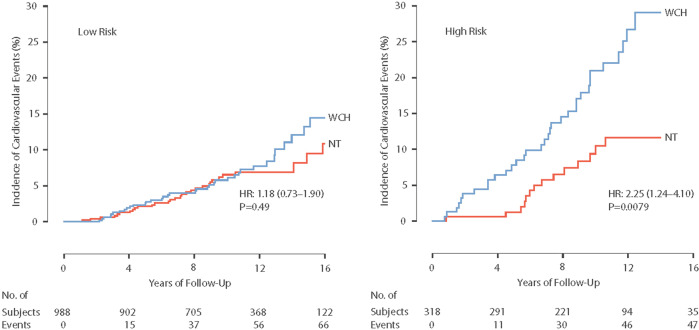
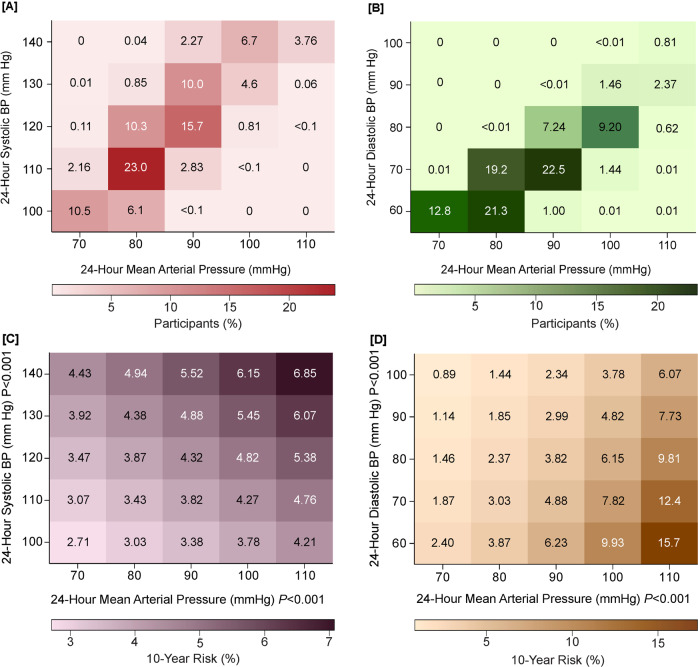
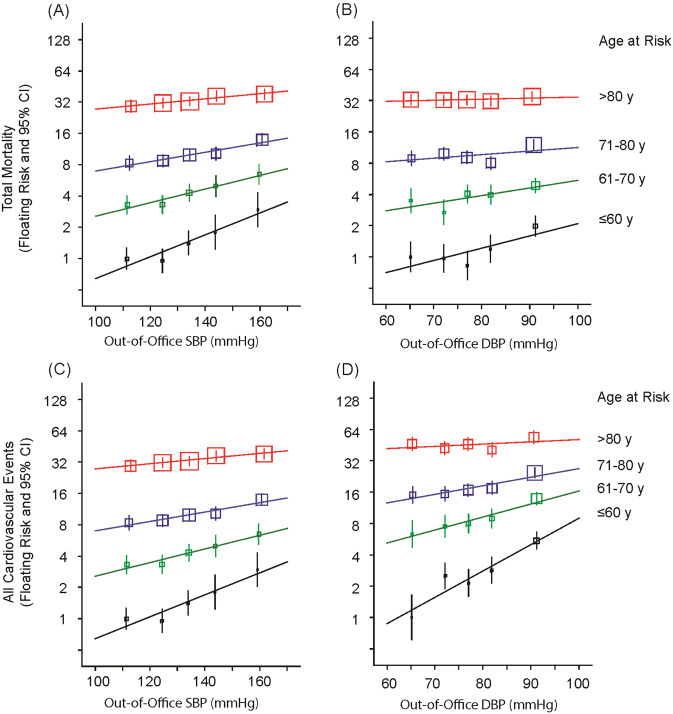
To assess in individual-person meta-analyses how out-of-office blood pressure (BP) contributes to risk stratification and the management of hypertension, an international consortium set up the International Databases on Ambulatory (IDACO) and Home (IDHOCO) Blood Pressure in Relation to Cardiovascular Outcome. This review summarizes key findings of recent IDACO/IDHOCO articles. Among various BP indexes derived from office and ambulatory BP recordings, the 24-h and nighttime BP level were the best predictors of adverse health outcomes. Second, using the 10-year cardiovascular risk associated with guideline-endorsed office BP thresholds as reference, corresponding thresholds were derived for home and ambulatory BP. Stratified by the underlying cardiovascular risk, the rate of cardiovascular events in white-coat hypertensive patients and matched normotensive controls were not substantially different. The observation that masked hypertension carries a high cardiovascular risk was replicated in Nigerian Blacks, using home BP monitoring. The thresholds for 24-h mean arterial pressure, i.e., the BP component measured by oscillometric devices, delineating normotension, elevated BP and hypertension were <90, 90 to 92 and ≥92 mmHg. At young age, the absolute risk associated with out-of-office BP was low, but the relative risk was high, whereas with advancing age, the relative risk decreased and the absolute risk increased. Using pulse pressure as an exemplary case, the relative risks of death, cardiovascular endpoints and stroke decreased over 3-fold from 55 to 75 years of age, whereas in contrast absolute risk rose 3-fold. In conclusion, IDACO/IDHOCO forcefully support the notion that the pressing need to curb the hypertension pandemic cannot be met without out-of-the-office BP monitoring.
为了在个体患者的荟萃分析中评估非诊室血压(BP)在危险分层和高血压管理中的作用,一个国际联合会建立了国际动态血压数据库(IDACO)和家庭血压数据库(IDHOCO)以评估血压与心血管结局的关系。本综述总结了最近 IDACO/IDHOCO 文章的主要发现。在从诊室和动态血压记录中得出的各种 BP 指标中,24 小时和夜间 BP 水平是不良健康结局的最佳预测指标。其次,以指南推荐的诊室 BP 阈值相关的 10 年心血管风险为参考,推导出了家庭和动态血压的相应阈值。根据潜在的心血管风险分层,白大衣高血压患者和匹配的正常血压对照者的心血管事件发生率没有显著差异。在家中使用血压监测,在尼日利亚黑人中复制了隐匿性高血压具有高心血管风险的观察结果。24 小时平均动脉压(即由振荡测量设备测量的 BP 成分)的阈值,界定正常血压、升高的血压和高血压的范围分别为<90、90-92 和≥92mmHg。在年轻时期,非诊室 BP 相关的绝对风险较低,但相对风险较高,而随着年龄的增长,相对风险降低,绝对风险增加。以脉压为例,死亡、心血管终点和中风的相对风险从 55 岁到 75 岁下降了 3 倍以上,而绝对风险增加了 3 倍。总之,IDACO/IDHOCO 有力地支持了这样一种观点,即在不进行非诊室 BP 监测的情况下,遏制高血压流行的紧迫需求无法得到满足。