Research Unit Hypertension and Cardiovascular Epidemiology, KU Leuven Department of Cardiovascular Sciences, University of Leuven, Leuven, Belgium.
Laboratory of Neurosciences, Faculty of Medicine, University of Zulia, Maracaibo, Zulia, Venezuela.
Am J Hypertens. 2021 Sep 22;34(9):929-938. doi: 10.1093/ajh/hpab048.
Pulse pressure (PP) reflects the age-related stiffening of the central arteries, but no study addressed the management of the PP-related risk over the human lifespan.
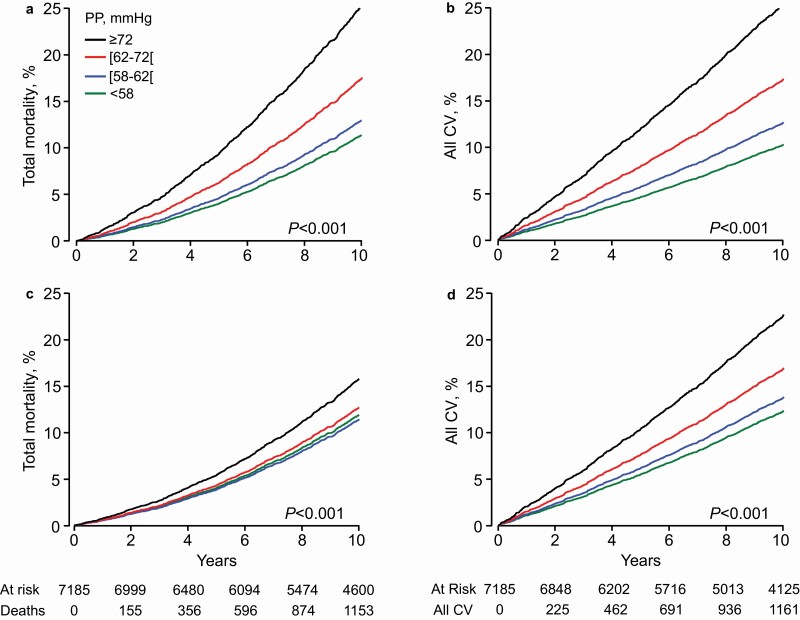
In 4,663 young (18-49 years) and 7,185 older adults (≥50 years), brachial PP was recorded over 24 hours. Total mortality and all major cardiovascular events (MACEs) combined were coprimary endpoints. Cardiovascular death, coronary events, and stroke were secondary endpoints.
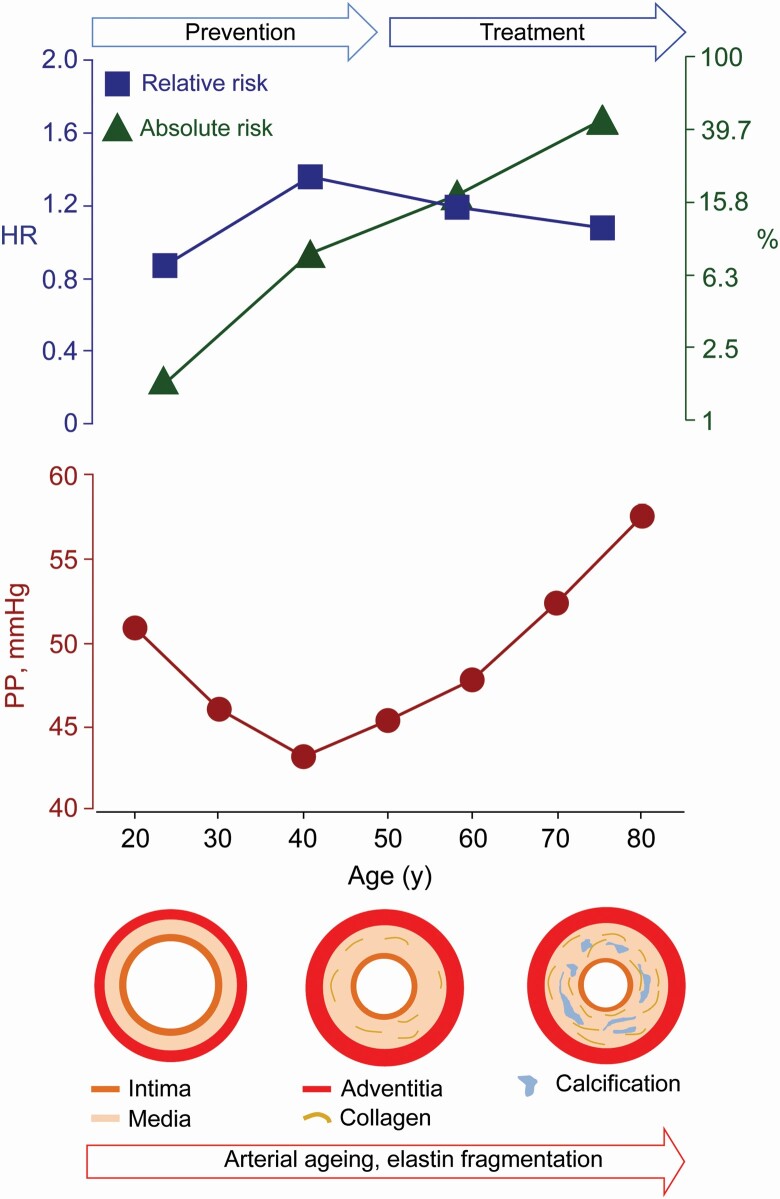
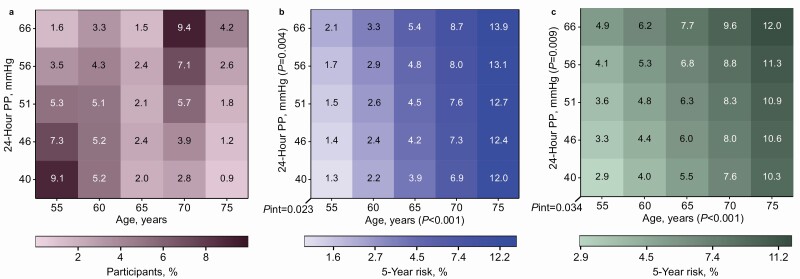
In young adults (median follow-up, 14.1 years; mean PP, 45.1 mm Hg), greater PP was not associated with absolute risk; the endpoint rates were ≤2.01 per 1,000 person-years. The adjusted hazard ratios expressed per 10-mm Hg PP increments were less than unity (P ≤ 0.027) for MACE (0.67; 95% confidence interval [CI], 0.47-0.96) and cardiovascular death (0.33; 95% CI, 0.11-0.75). In older adults (median follow-up, 13.1 years; mean PP, 52.7 mm Hg), the endpoint rates, expressing absolute risk, ranged from 22.5 to 45.4 per 1,000 person-years and the adjusted hazard ratios, reflecting relative risk, from 1.09 to 1.54 (P < 0.0001). The PP-related relative risks of death, MACE, and stroke decreased >3-fold from age 55 to 75 years, whereas absolute risk rose by a factor 3.
From 50 years onwards, the PP-related relative risk decreases, whereas absolute risk increases. From a lifecourse perspective, young adulthood provides a window of opportunity to manage risk factors and prevent target organ damage as forerunner of premature death and MACE. In older adults, treatment should address absolute risk, thereby extending life in years and quality.
脉压(PP)反映了中心动脉与年龄相关的僵硬程度,但尚无研究探讨人类寿命中与 PP 相关的风险管理。
在 4663 名年轻(18-49 岁)和 7185 名老年(≥50 岁)成年人中,24 小时内记录肱动脉 PP。总死亡率和所有主要心血管事件(MACE)的合并是共同的主要终点。心血管死亡、冠状动脉事件和中风是次要终点。
在年轻成年人(中位随访时间 14.1 年;平均 PP 为 45.1mmHg)中,较大的 PP 与绝对风险无关;终点发生率为≤每 1000 人年 2.01 例。每增加 10mmHg PP 的调整后的危险比均小于 1(P≤0.027),MACE(0.67;95%置信区间[CI],0.47-0.96)和心血管死亡(0.33;95%CI,0.11-0.75)。在老年成年人(中位随访时间 13.1 年;平均 PP 为 52.7mmHg)中,表达绝对风险的终点发生率范围为每 1000 人年 22.5-45.4 例,反映相对风险的调整后危险比范围为 1.09-1.54(P<0.0001)。PP 相关的死亡、MACE 和中风风险从 55 岁到 75 岁降低了>3 倍,而绝对风险增加了 3 倍。
从 50 岁开始,PP 相关的相对风险降低,而绝对风险增加。从生命过程的角度来看,成年早期为管理危险因素和预防目标器官损伤提供了机会,因为这是早逝和 MACE 的先兆。在老年成年人中,治疗应针对绝对风险,从而延长生命年限和质量。