Research Center, CIUSSS du Nord-de-l'île-de-Montréal, University of Montreal, Montreal, QC, Canada.
Nephrology Division, NYU Langone Health, NYU Grossman School of Medicine, New York, NY, USA.
Crit Care. 2023 Feb 10;27(1):56. doi: 10.1186/s13054-022-04227-2.
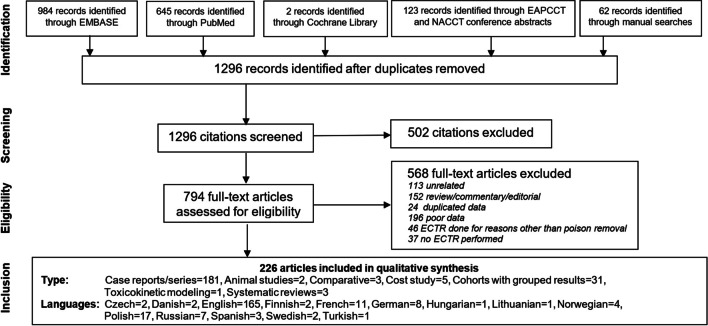
Ethylene glycol (EG) is metabolized into glycolate and oxalate and may cause metabolic acidemia, neurotoxicity, acute kidney injury (AKI), and death. Historically, treatment of EG toxicity included supportive care, correction of acid-base disturbances and antidotes (ethanol or fomepizole), and extracorporeal treatments (ECTRs), such as hemodialysis. With the wider availability of fomepizole, the indications for ECTRs in EG poisoning are debated. We conducted systematic reviews of the literature following published EXTRIP methods to determine the utility of ECTRs in the management of EG toxicity. The quality of the evidence and the strength of recommendations, either strong ("we recommend") or weak/conditional ("we suggest"), were graded according to the GRADE approach. A total of 226 articles met inclusion criteria. EG was assessed as dialyzable by intermittent hemodialysis (level of evidence = B) as was glycolate (Level of evidence = C). Clinical data were available for analysis on 446 patients, in whom overall mortality was 18.7%. In the subgroup of patients with a glycolate concentration ≤ 12 mmol/L (or anion gap ≤ 28 mmol/L), mortality was 3.6%; in this subgroup, outcomes in patients receiving ECTR were not better than in those who did not receive ECTR. The EXTRIP workgroup made the following recommendations for the use of ECTR in addition to supportive care over supportive care alone in the management of EG poisoning (very low quality of evidence for all recommendations): i) Suggest ECTR if fomepizole is used and EG concentration > 50 mmol/L OR osmol gap > 50; or ii) Recommend ECTR if ethanol is used and EG concentration > 50 mmol/L OR osmol gap > 50; or iii) Recommend ECTR if glycolate concentration is > 12 mmol/L or anion gap > 27 mmol/L; or iv) Suggest ECTR if glycolate concentration 8-12 mmol/L or anion gap 23-27 mmol/L; or v) Recommend ECTR if there are severe clinical features (coma, seizures, or AKI). In most settings, the workgroup recommends using intermittent hemodialysis over other ECTRs. If intermittent hemodialysis is not available, CKRT is recommended over other types of ECTR. Cessation of ECTR is recommended once the anion gap is < 18 mmol/L or suggested if EG concentration is < 4 mmol/L. The dosage of antidotes (fomepizole or ethanol) needs to be adjusted during ECTR.
乙二醇(EG)代谢为乙醇酸和草酸,可能导致代谢性酸中毒、神经毒性、急性肾损伤(AKI)和死亡。历史上,EG 毒性的治疗包括支持性治疗、酸碱紊乱的纠正和解毒剂(乙醇或 fomepizole)以及体外治疗(ECTR),如血液透析。随着 fomepizole 的广泛应用,EG 中毒时 ECTR 的适应证存在争议。我们按照已发表的 EXTRIP 方法对文献进行了系统评价,以确定 ECTR 在 EG 毒性管理中的应用。根据 GRADE 方法,对证据质量和建议强度(强“我们建议”或弱/有条件“我们建议”)进行分级。共有 226 篇文章符合纳入标准。EG 通过间歇性血液透析(证据水平=B)和乙醇酸(证据水平=C)被评估为可透析。对 446 名患者的临床数据进行了分析,其中总体死亡率为 18.7%。在血乙醇酸浓度≤12mmol/L(或阴离子间隙≤28mmol/L)的亚组中,死亡率为 3.6%;在这个亚组中,接受 ECTR 治疗的患者的结局并不优于未接受 ECTR 治疗的患者。EXTRIP 工作组除了支持性治疗外,还提出了在 EG 中毒管理中使用 ECTR 的以下建议(所有建议的证据质量均非常低):i)如果使用 fomepizole 且 EG 浓度>50mmol/L 或 osmol 间隙>50,则建议使用 ECTR;或 ii)如果使用乙醇且 EG 浓度>50mmol/L 或 osmol 间隙>50,则建议使用 ECTR;或 iii)如果乙醇酸浓度>12mmol/L 或阴离子间隙>27mmol/L,则建议使用 ECTR;或 iv)如果乙醇酸浓度为 8-12mmol/L 或阴离子间隙为 23-27mmol/L,则建议使用 ECTR;或 v)如果存在严重的临床特征(昏迷、癫痫发作或 AKI),则建议使用 ECTR。在大多数情况下,工作组建议使用间歇性血液透析代替其他 ECTR。如果无法进行间歇性血液透析,则建议使用 CKRT 代替其他类型的 ECTR。一旦阴离子间隙<18mmol/L,或 EG 浓度<4mmol/L,建议停止 ECTR。ECTR 期间需要调整解毒剂(fomepizole 或乙醇)的剂量。