Division of Nephrology, Verdun Hospital, University of Montreal , Montreal, QC , Canada.
Clin Toxicol (Phila). 2014 Dec;52(10):993-1004. doi: 10.3109/15563650.2014.973572. Epub 2014 Oct 30.
The Extracorporeal Treatments in Poisoning (EXTRIP) workgroup was created to provide evidence and consensus-based recommendations on the use of extracorporeal treatments (ECTRs) in poisoning.
To perform a systematic review and provide clinical recommendations for ECTR in carbamazepine poisoning.
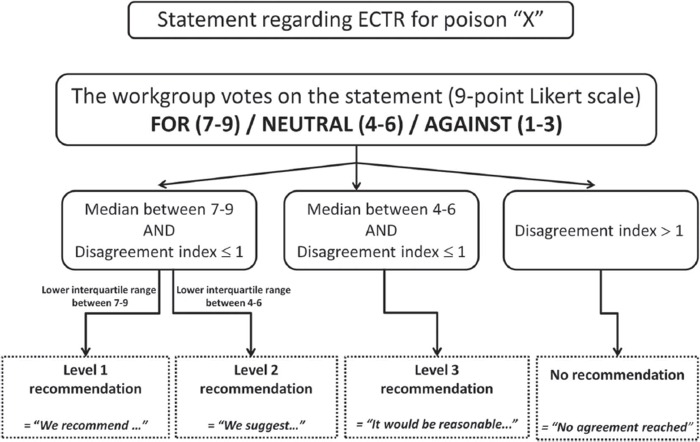
After a systematic literature search, the subgroup extracted the data and summarized the findings following a pre-determined format. The entire workgroup voted via a two-round modified Delphi method to reach a consensus on voting statements, using a RAND/UCLA Appropriateness Method to quantify disagreement. Anonymous votes were compiled, returned, and discussed in person. A second vote determined the final recommendations.
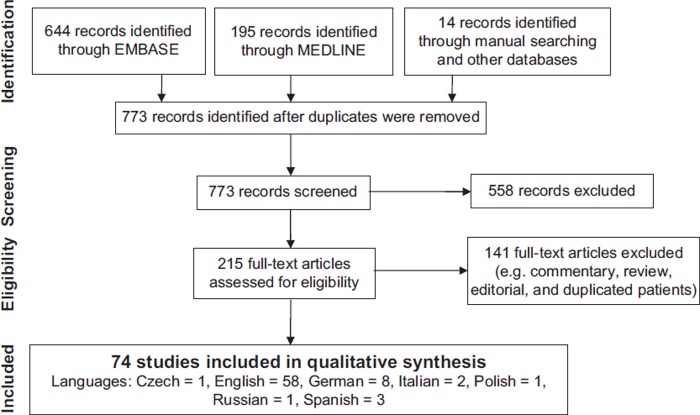
Seventy-four articles met inclusion criteria. Articles included case reports, case series, descriptive cohorts, pharmacokinetic studies, and in-vitro studies; two poor-quality observational studies were identified, yielding a very low quality of evidence for all recommendations. Data on 173 patients, including 6 fatalities, were reviewed. The workgroup concluded that carbamazepine is moderately dialyzable and made the following recommendations: ECTR is suggested in severe carbamazepine poisoning (2D). ECTR is recommended if multiple seizures occur and are refractory to treatment (1D), or if life-threatening dysrhythmias occur (1D). ECTR is suggested if prolonged coma or respiratory depression requiring mechanical ventilation are present (2D) or if significant toxicity persists, particularly when carbamazepine concentrations rise or remain elevated, despite using multiple-dose activated charcoal (MDAC) and supportive measures (2D). ECTR should be continued until clinical improvement is apparent (1D) or the serum carbamazepine concentration is below 10 mg/L (42 the μ in μmol/L looks weird.) (2D). Intermittent hemodialysis is the preferred ECTR (1D), but both intermittent hemoperfusion (1D) or continuous renal replacement therapies (3D) are alternatives if hemodialysis is not available. MDAC therapy should be continued during ECTR (1D).
Despite the low quality of the available clinical evidence and the high protein binding capacity of carbamazepine, the workgroup suggested extracorporeal removal in cases of severe carbamazepine poisoning.
体外治疗中毒(EXTRIP)工作组的成立旨在提供有关体外治疗(ECTR)在中毒中的使用的证据和基于共识的建议。
对卡马西平中毒的 ECTR 进行系统评价并提供临床建议。
经过系统的文献检索,子组按照预先确定的格式提取数据并总结结果。整个工作组通过两轮修改后的 Delphi 方法对投票声明进行投票,使用 RAND/UCLA 适宜性方法量化分歧。匿名投票被编译、返回并亲自讨论。第二次投票确定了最终建议。
74 篇文章符合纳入标准。文章包括病例报告、病例系列、描述性队列、药代动力学研究和体外研究;确定了两项低质量的观察性研究,所有建议的证据质量均非常低。共回顾了 173 名患者的数据,包括 6 例死亡。工作组得出结论,卡马西平可适度透析,并提出了以下建议:在严重卡马西平中毒时建议进行 ECTR(2D)。如果发生多次且对治疗有抗药性的癫痫发作(1D),或者出现危及生命的心律失常(1D),则建议进行 ECTR。如果存在长时间昏迷或需要机械通气的呼吸抑制(2D),或者存在明显毒性持续存在,特别是当卡马西平浓度升高或仍然升高时,尽管使用了多次剂量活性炭(MDAC)和支持措施(2D),则建议进行 ECTR。应继续进行 ECTR,直到临床症状明显改善(1D)或血清卡马西平浓度低于 10 mg/L(42 中 μ 在 μmol/L 中看起来很奇怪。)(2D)。间歇性血液透析是首选的 ECTR(1D),但如果无法进行血液透析,则可以选择间歇性血液灌流(1D)或连续肾脏替代疗法(3D)作为替代方法。在进行 ECTR 期间应继续进行 MDAC 治疗(1D)。
尽管现有临床证据质量较低,且卡马西平的蛋白结合能力较高,但工作组建议在严重卡马西平中毒的情况下进行体外清除。