Department of Epidemiology and Health Statistics, School of Public Health, Lanzhou University, Lanzhou 730000, China.
Int J Environ Res Public Health. 2023 Jan 18;20(3):1728. doi: 10.3390/ijerph20031728.
Although several studies have examined the association between chronic kidney disease (CKD) and hyperuricemia (HUA), the direction of the association remains unclear. We aimed to investigate whether there was a bidirectional association between them.
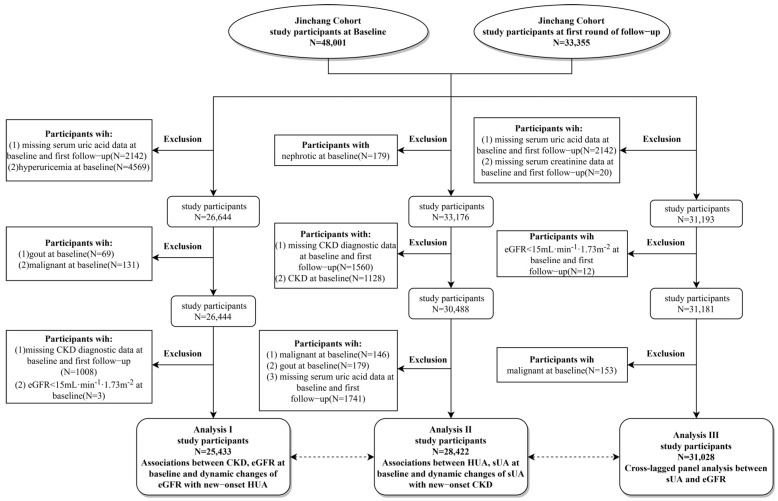
The present study was conducted in three analyses. Analysis I included 25,433 participants free of HUA at baseline to evaluate the associations between CKD and estimated glomerular filtration rate (eGFR) with incident HUA. Analysis II had 28,422 participants free of CKD at baseline to analyze the relationships between HUA and serum uric acid (sUA) with new-onset CKD. Cox proportional hazards regression models were applied to evaluate the association involved in Analysis I and II. Analysis III included 31,028 participants with complete data and further dissected the bidirectional association between sUA and eGFR using cross-lag models.
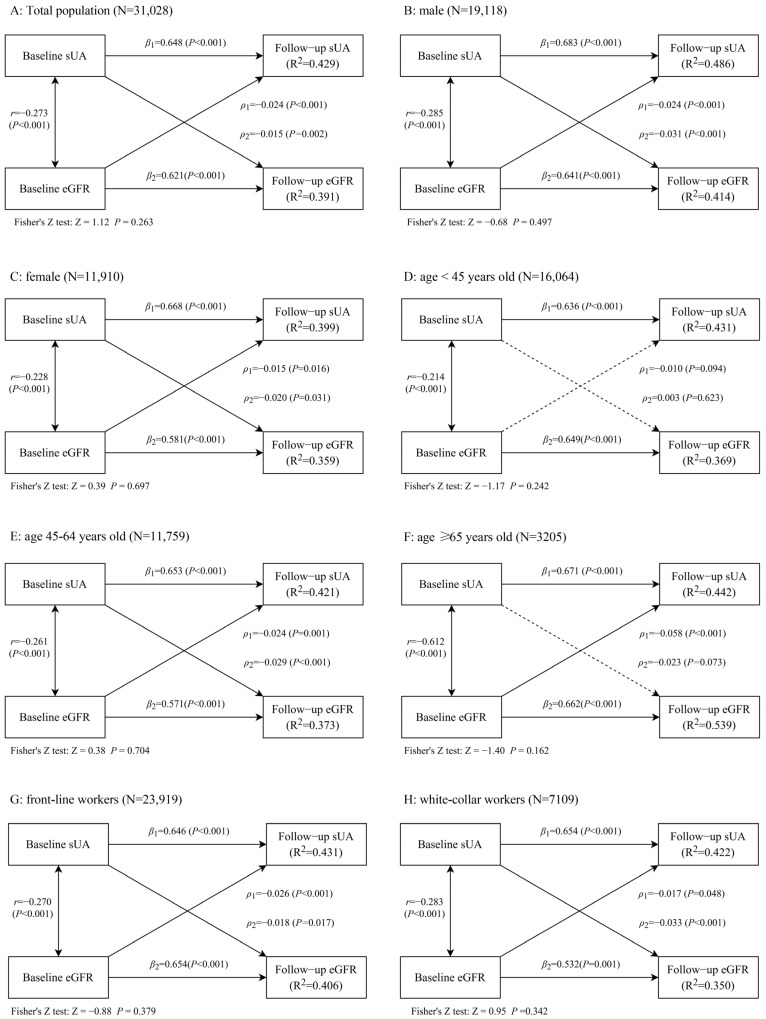
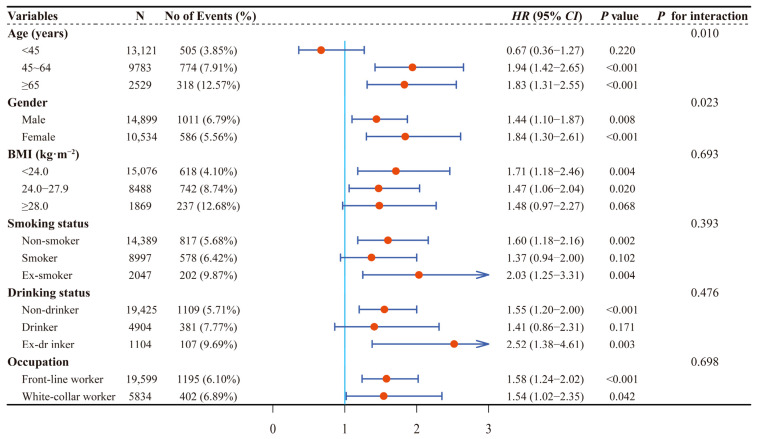
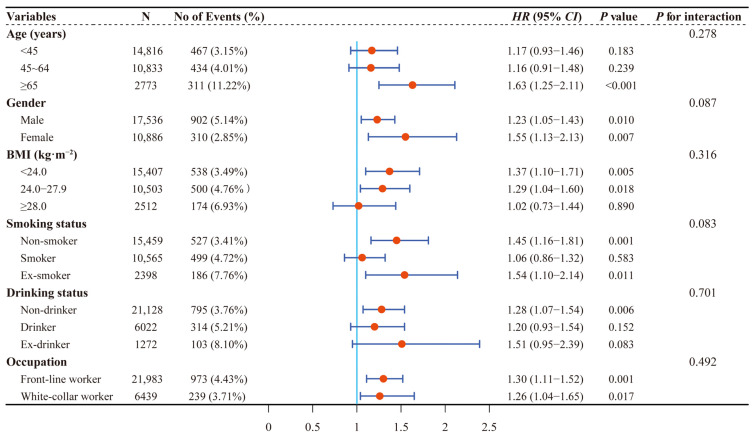
New-onset HUA and CKD were observed in the first round of the follow-up study among 1597 and 1212 participants, respectively. A significantly higher risk of HUA was observed in individuals with CKD compared to individuals without CKD ( = 1.58, 95% : 1.28-1.95). The adjusted s (95% s) of HUA were 3.56 (2.50-5.05) for the participants in the group of eGFR less than 60 mL·min·1.73 m, 1.61 (1.42-1.83) for those in the group of eGFR between 60 and 90 mL·min·1.73 m, and 1.74 (1.42-2.14) for those in the group of eGFR more than 120 mL·min·1.73 m, compared with the group of eGFR between 90 and 120 mL·min·1.73 m. A higher risk of CKD was also observed in individuals with HUA compared to individuals without HUA ( = 1.28, 95% : 1.12-1.47). Compared with the first quintile of sUA, the adjusted (95% ) of CKD was 1.24 (1.01-1.51) for the participants in the fourth quantile. There was a bidirectional relationship between sUA and eGFR, with the path coefficients ( = -0.024, < 0.001) from baseline eGFR to follow-up sUA and the path coefficients ( = -0.015, = 0.002) from baseline sUA to follow-up eGFR.
The present study indicated that CKD and HUA were closely associated, and there was a bidirectional relationship between sUA and eGFR.
尽管已有多项研究探讨了慢性肾脏病(CKD)与高尿酸血症(HUA)之间的关系,但两者之间的关联方向仍不明确。本研究旨在探究两者之间是否存在双向关联。
本研究共进行了三项分析。分析 I 纳入了 25433 名基线时无 HUA 的参与者,以评估 CKD 与估算肾小球滤过率(eGFR)与新发 HUA 之间的关联。分析 II 纳入了 28422 名基线时无 CKD 的参与者,以分析 HUA 与血清尿酸(sUA)与新发 CKD 之间的关系。采用 Cox 比例风险回归模型评估分析 I 和 II 中涉及的关联。分析 III 纳入了 31028 名数据完整的参与者,并进一步使用交叉滞后模型剖析了 sUA 与 eGFR 之间的双向关联。
在第一轮随访研究中,1597 名参与者出现新发 HUA,1212 名参与者出现新发 CKD。与无 CKD 的参与者相比,CKD 患者新发 HUA 的风险显著更高( = 1.58,95%:1.28-1.95)。与 eGFR 介于 90-120 mL·min·1.73 m 之间的参与者相比,eGFR 小于 60 mL·min·1.73 m 组参与者的 HUA 调整后 s 值(95% s 值)为 3.56(2.50-5.05),eGFR 介于 60-90 mL·min·1.73 m 组参与者的 HUA 调整后 s 值为 1.61(1.42-1.83),eGFR 大于 120 mL·min·1.73 m 组参与者的 HUA 调整后 s 值为 1.74(1.42-2.14)。与无 HUA 的参与者相比,HUA 患者新发 CKD 的风险也显著更高( = 1.28,95%:1.12-1.47)。与 sUA 的第一分位数相比,第四分位数参与者的 CKD 调整后比值比(95% 比值比)为 1.24(1.01-1.51)。sUA 与 eGFR 之间存在双向关系,从基线 eGFR 到随访 sUA 的路径系数( = -0.024, < 0.001)和从基线 sUA 到随访 eGFR 的路径系数( = -0.015, = 0.002)。
本研究表明 CKD 和 HUA 密切相关,sUA 与 eGFR 之间存在双向关系。