Department of Pediatrics, Yonsei University Wonju College of Medicine, Wonju 26426, Republic of Korea.
Division of Pediatric Cardiology, Department of Pediatrics, Yonsei University College of Medicine, Seoul 03722, Republic of Korea.
Int J Environ Res Public Health. 2023 Jan 25;20(3):2191. doi: 10.3390/ijerph20032191.
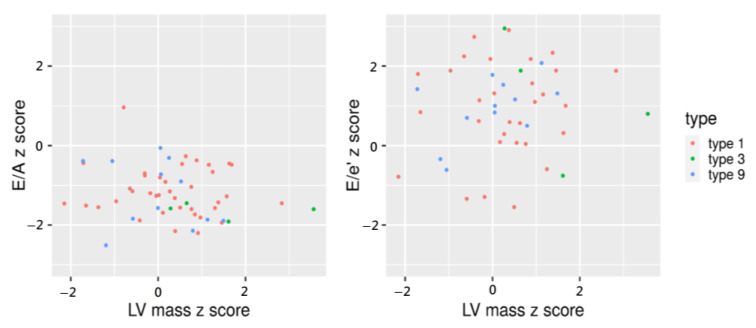
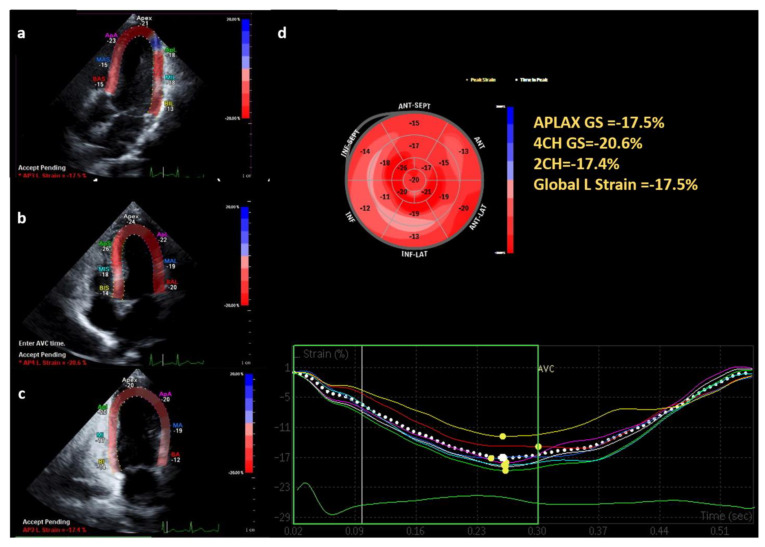
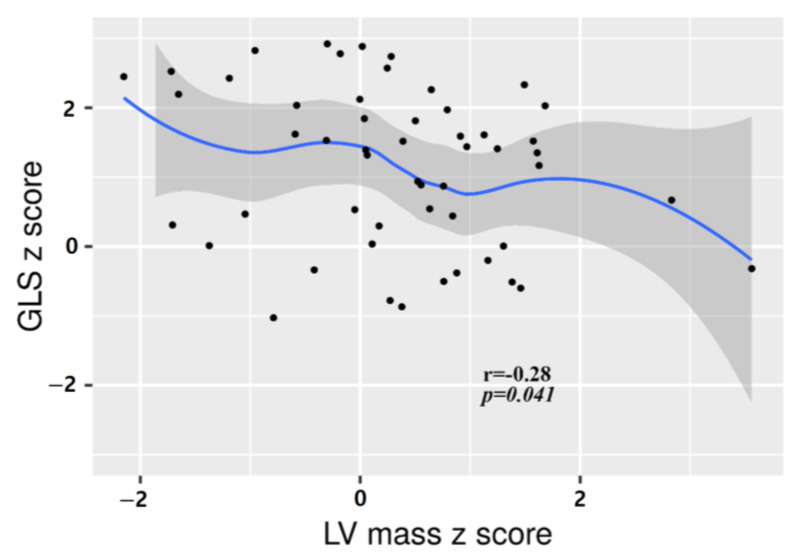
Glycogen storage disease (GSD) is a hereditary metabolic disorder caused by enzyme deficiency resulting in glycogen accumulation in the liver, muscle, heart, or kidney. GSD types II, III, IV, and IX are associated with cardiac involvement. However, cardiac manifestation in other GSD types is unclear. This study aimed to describe whether energy deprivation and the toxic effects of accumulated glycogen affect the heart of patients with GSD. We evaluated the left ventricle (LV) wall mass, LV systolic and diastolic function and myocardial strain with conventional echocardiography and two-dimensional speckle-tracking echocardiography (2D STE) in 62 patients with GSD type I, III, VI and IX who visited the Wonju Severance Hospital in 2021. Among the GSD patients, the echocardiographic parameters of 55 pediatrics were converted into z-scores and analyzed. Of the patients, 43 (62.3%), 7 (11.3%) and 12 (19.4%) patients were diagnosed with GSD type I, type III, and type IX, respectively. The median age was 9 years (range, 1-36 years), with 55 children under 18 years old and seven adults over 18 years. For the 55 pediatric patients, the echocardiographic parameters were converted into a z-score and analyzed. Multiple linear regression analysis showed that the BMI z-score ( = 0.022) and CK ( = 0.020) predicted increased LV mass z-score, regardless of GSD type. There was no difference in the diastolic and systolic functions according to myocardial thickness; however, 2D STE showed a negative correlation with the LV mass (r = -0.28, = 0.041). Given that patients with GSD tend to be overweight, serial evaluation with echocardiography might be required for all types of GSD.
糖原贮积病(GSD)是一种遗传性代谢紊乱,由酶缺乏引起,导致肝、肌肉、心脏或肾脏中糖原积累。GSD 型 II、III、IV 和 IX 与心脏受累有关。然而,其他 GSD 型的心脏表现尚不清楚。本研究旨在描述能量剥夺和堆积糖原的毒性作用是否会影响 GSD 患者的心脏。我们评估了 2021 年在原州Severance 医院就诊的 62 例 GSD 型 I、III、VI 和 IX 患者的左心室(LV)壁质量、LV 收缩和舒张功能以及心肌应变,采用常规超声心动图和二维斑点追踪超声心动图(2D STE)。在 GSD 患者中,55 名儿科患者的超声心动图参数转换为 z 评分并进行分析。患者中,43 例(62.3%)、7 例(11.3%)和 12 例(19.4%)分别诊断为 GSD 型 I、III 和 IX。中位年龄为 9 岁(范围,1-36 岁),55 例为 18 岁以下儿童,7 例为 18 岁以上成人。对于 55 名儿科患者,超声心动图参数转换为 z 评分并进行分析。多元线性回归分析显示,BMI z 评分( = 0.022)和 CK( = 0.020)可预测 LV 质量 z 评分增加,与 GSD 类型无关。心肌厚度不同,舒张和收缩功能无差异;然而,2D STE 与 LV 质量呈负相关(r = -0.28, = 0.041)。鉴于 GSD 患者往往超重,可能需要对所有类型的 GSD 进行超声心动图的连续评估。