Charaf Zohra, Tanaka Kaoru, Wellens Francis, Nijs Jan, Van Loo Ines, Argacha Jean-Francois, La Meir Mark
Department of Cardiac Surgery, UZ Brussel, Brussels, Belgium.
Department of Radiology, UZ Brussel, Brussels, Belgium.
Interdiscip Cardiovasc Thorac Surg. 2023 Jan 9;36(1). doi: 10.1093/icvts/ivac286.
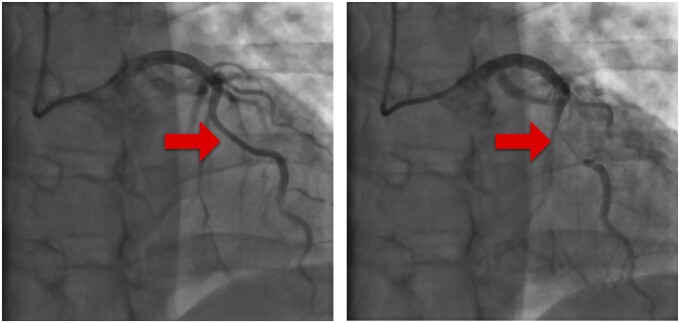
Myocardial bridging is mostly diagnosed as an incidental imaging finding but can result in severe vessel compression and significant clinical adverse complications. Since there is still an ongoing debate when to propose surgical unroofing, we studied a group of patients where this was performed as an isolated procedure.
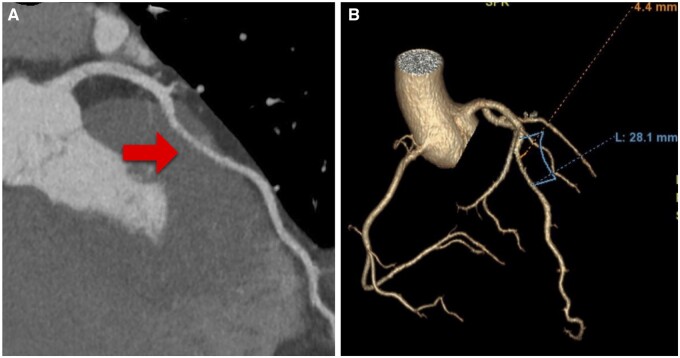
In 16 patients (38.9 ± 15.7 years, 75% men) who had surgical unroofing for symptomatic isolated myocardial bridges of the left anterior descending artery, we retrospectively analysed symptomatology, medication, imaging modalities used, operative techniques, complications and long-term outcome. Computed tomographic fractional flow reserve was calculated to understand its potential value for decision-making.
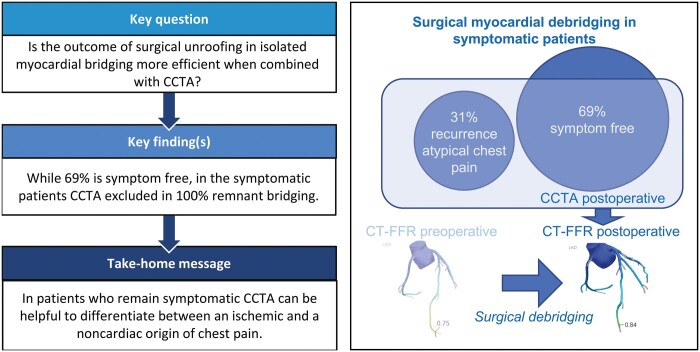
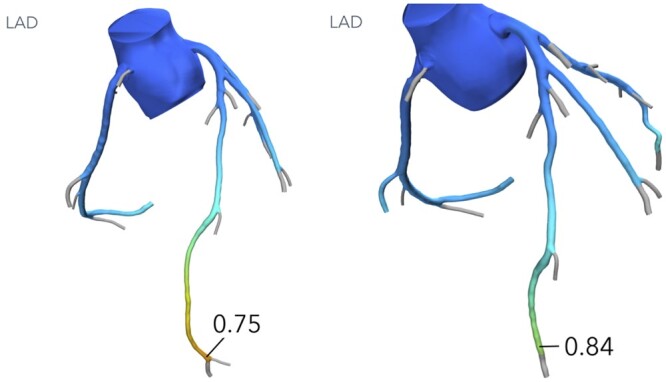
Most procedures were performed on-pump (75%, mean cardiopulmonary bypass 56.5 ± 27.9 min, mean aortic cross-clamping 36.4 ± 19.7 min). Three patients needed a left internal mammary artery bypass since the artery dived inside the ventricle. There were no major complications or deaths. The mean follow-up was 5.5 years. Although there was a dramatic improvement in symptoms, still 31% experienced atypical chest pain at various moments during follow-up. Postoperative radiological control was performed in 88%, showing no residual compression or recurrent myocardial bridge and patent bypass if performed. All postoperative computed tomographic flow calculations (7) showed a normalization of coronary flow.
Surgical unroofing for symptomatic isolated myocardial bridging is a safe procedure. Patient selection remains difficult but introducing standard coronary computed tomographic angiography with flow calculations could be helpful in preoperative decision-making and during follow-up.
心肌桥大多作为偶然的影像学发现而被诊断,但可导致严重的血管受压及显著的临床不良并发症。由于在何时建议进行外科心肌桥松解术方面仍存在争议,我们研究了一组接受该手术作为单独操作的患者。
对16例(年龄38.9±15.7岁,75%为男性)因症状性孤立性左前降支心肌桥而接受外科心肌桥松解术的患者,我们回顾性分析了症状、用药情况、所使用的影像学检查方法、手术技术、并发症及长期预后。计算计算机断层扫描血流储备分数以了解其在决策中的潜在价值。
大多数手术在体外循环下进行(75%),平均体外循环时间56.5±27.9分钟,平均主动脉阻断时间36.4±19.7分钟。3例患者因动脉潜入心室内而需要行左乳内动脉搭桥术。无重大并发症或死亡。平均随访时间为5.5年。尽管症状有显著改善,但仍有31%的患者在随访期间不同时间出现非典型胸痛。88%的患者进行了术后影像学检查,结果显示无残余压迫或复发性心肌桥,若进行了搭桥术则搭桥血管通畅。所有术后计算机断层扫描血流计算(7例)均显示冠状动脉血流恢复正常。
对症状性孤立性心肌桥进行外科心肌桥松解术是一种安全的手术。患者选择仍然困难,但引入标准的冠状动脉计算机断层扫描血管造影并进行血流计算可能有助于术前决策及随访。