Adams Leslie B, Zimmer Catherine, Progovac Ana M, Creedon Timothy, Rodgers Caryn R R, Sonik Rajan A, Cook Benjamin Lê
Department of Mental Health, Johns Hopkins Bloomberg School of Public Health, USA.
Department of Sociology, University of North Carolina at Chapel Hill, USA.
SSM Ment Health. 2022 Dec;2. doi: 10.1016/j.ssmmh.2022.100105. Epub 2022 May 4.
Discrimination is experienced across demographic attributes (e.g., race and gender) and vantage points (e.g., personal and vicarious), yet few studies have classified these different experiences of discrimination within healthcare systems. Moreover, which discriminatory experiences have greater influence on patient-reported quality outcomes remains poorly understood. To address these gaps, we used latent class analysis (LCA) to identify typologies of past experiences with healthcare discrimination among adults with depression-who experience more frequent and stigmatizing healthcare interactions than the general population-and assess the relationship between class membership and current ratings of patient-reported quality outcomes.
We surveyed a nationally representative sample of adults with depression (n = 803) to assess past experiences of discrimination by medical providers in terms of both the characteristics targeted for discrimination and whether healthcare discrimination was experienced personally or by friends and family members. We conducted an LCA to identify discrimination-exposure classes and a modified Poisson regression to identify associations between class membership and patient-reported quality outcomes (e.g., overall medical provider quality, respect, clear communication, and careful listening), while adjusting for covariates.
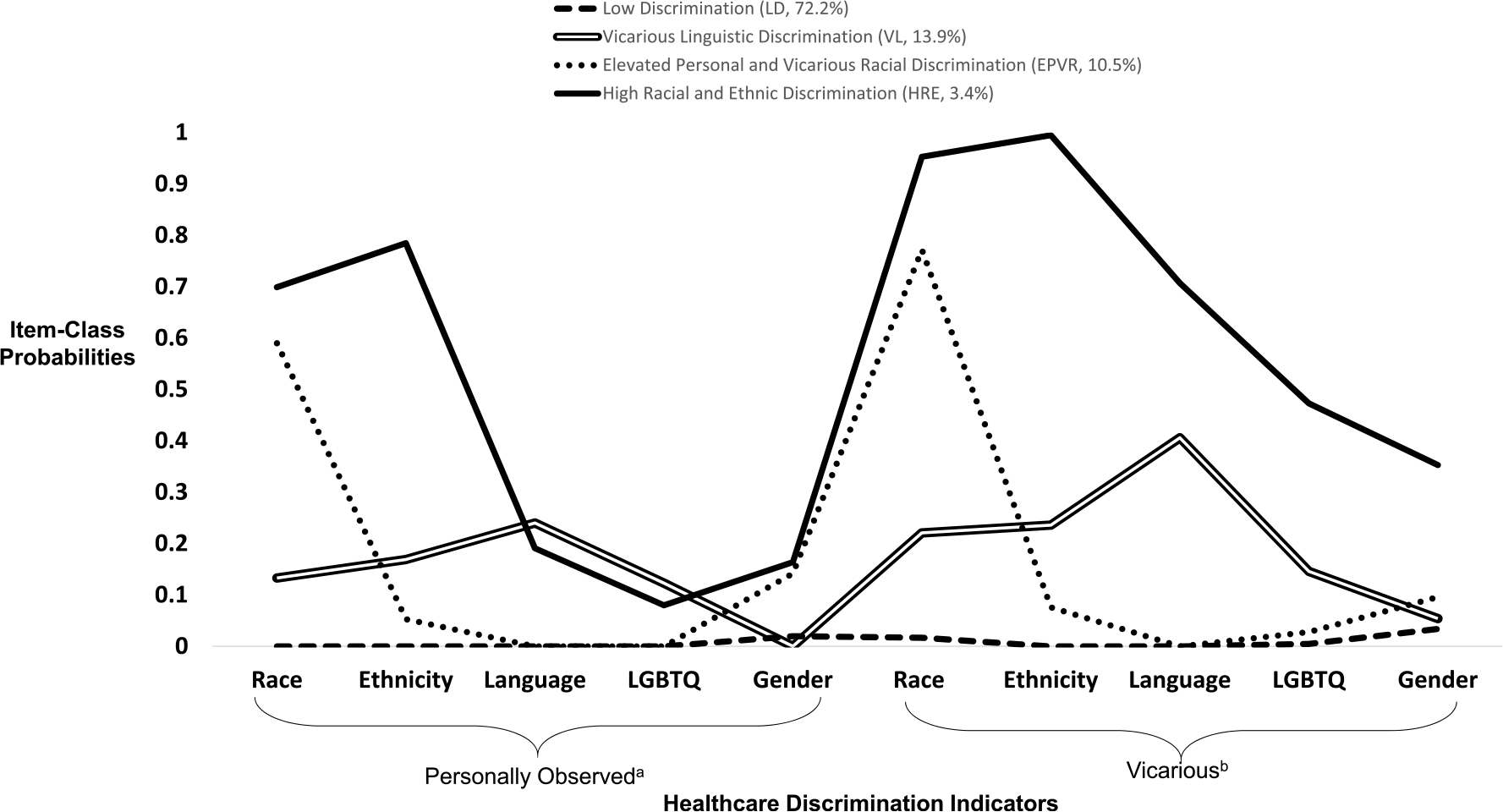
We identified four latent classes of healthcare discrimination: low discrimination (LD; referent class: 72.2% of total sample), vicarious linguistic discrimination (VL; 13.9%), elevated personal and vicarious racial discrimination (EPVR; 10.5%), and high racial/ethnic discrimination (HRE; 3.4%). Compared to those in the LD class, individuals in the EPVR class had higher rates of reporting their current medical provider's respect and careful listening skills as sometimes or never, (Respect aIRR: 1.90, 95% CI: 1.05-3.42; Listening aIRR: 2.18, 95% CI: 1.29-3.66). Those in the HRE class reported higher rates of reporting their medical provider's quality and communication as poor or fair and lower ratings of careful listening (Quality aIRR: 2.06, 95% CI: 1.08-3.93; Communication aIRR: 1.97, 95% CI: 1.00-3.63; Listening aIRR: 2.41, 95% CI: 1.27-4.59), compared to those in the LD class. Those in the VL class had higher rates of reporting that their medical provider never or sometimes respected or carefully listened to them (Respect aIRR: 2.12, 95% CI: 1.20-3.72; Listening aIRR:1.67, 95% CI:1.03-2.71) than those in, the LD class.
Healthcare organizations committed to providing equitable patient care should establish more robust quality improvement approaches to prevent discrimination at the medical provider level as well as structures of accountability to reconcile previously embedded social inequities within the healthcare system.
歧视存在于各种人口统计学特征(如种族和性别)以及不同视角(如个人经历和间接经历)之中,但很少有研究对医疗系统内这些不同的歧视经历进行分类。此外,哪些歧视经历对患者报告的质量结果有更大影响仍知之甚少。为了填补这些空白,我们使用潜在类别分析(LCA)来识别抑郁症成年人过去的医疗歧视经历类型——他们比普通人群经历更频繁且带有污名化的医疗互动——并评估类别归属与患者报告的当前质量结果评分之间的关系。
我们对全国具有代表性的抑郁症成年人样本(n = 803)进行了调查,以评估医疗服务提供者过去在歧视目标特征方面的歧视经历,以及医疗歧视是个人经历还是朋友和家人经历。我们进行了潜在类别分析以识别歧视暴露类别,并进行了修正泊松回归以识别类别归属与患者报告的质量结果(如医疗服务提供者的总体质量、尊重、清晰沟通和认真倾听)之间的关联,同时对协变量进行调整。
我们识别出了四类医疗歧视潜在类别:低歧视(LD;参照类别:占总样本的72.2%)、间接语言歧视(VL;13.9%)、个人和间接种族歧视加剧(EPVR;10.5%)以及高种族/族裔歧视(HRE;3.4%)。与LD类别中的个体相比,EPVR类别中的个体报告其当前医疗服务提供者有时或从不具备尊重和认真倾听技能的比例更高(尊重调整发病率比:1.90,95%置信区间:1.05 - 3.42;倾听调整发病率比:2.18,95%置信区间:1.29 - 3.66)。与LD类别中的个体相比,HRE类别中的个体报告其医疗服务提供者质量和沟通为差或一般的比例更高,而认真倾听评分更低(质量调整发病率比:2.06,95%置信区间:1.08 - 3.93;沟通调整发病率比:1.97,95%置信区间:1.00 - 3.63;倾听调整发病率比:2.41,95%置信区间:1.27 - 4.59)。与LD类别中的个体相比,VL类别中的个体报告其医疗服务提供者从不或有时尊重或认真倾听他们的比例更高(尊重调整发病率比:2.12,95%置信区间:1.20 - 3.72;倾听调整发病率比:1.67,95%置信区间:1.03 - 2.71)。
致力于提供公平患者护理的医疗机构应建立更强大的质量改进方法,以防止医疗服务提供者层面的歧视,并建立问责机制,以消除医疗系统中先前存在的社会不平等现象。