Department of Surgery, University of Miami Health System, Miami, FL, USA.
Department of Surgery, New York University Langone Health, New York, USA.
J Cardiothorac Surg. 2023 Feb 24;18(1):79. doi: 10.1186/s13019-023-02168-7.
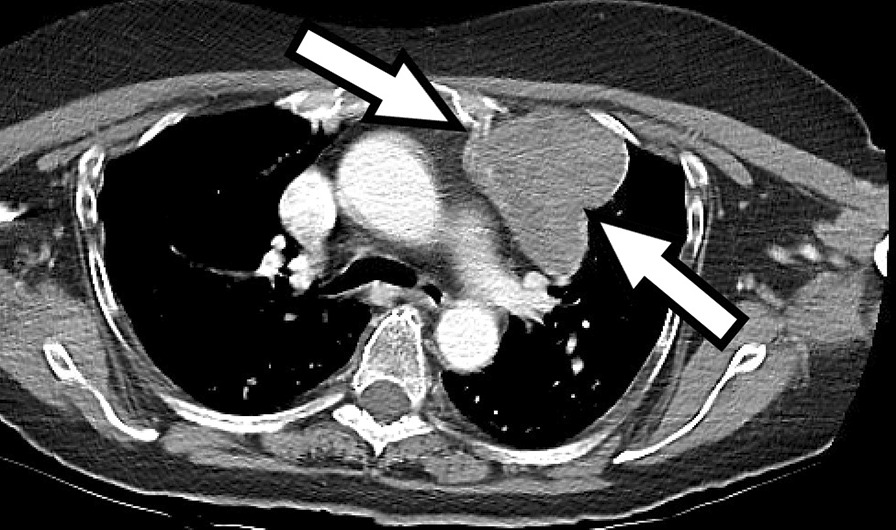
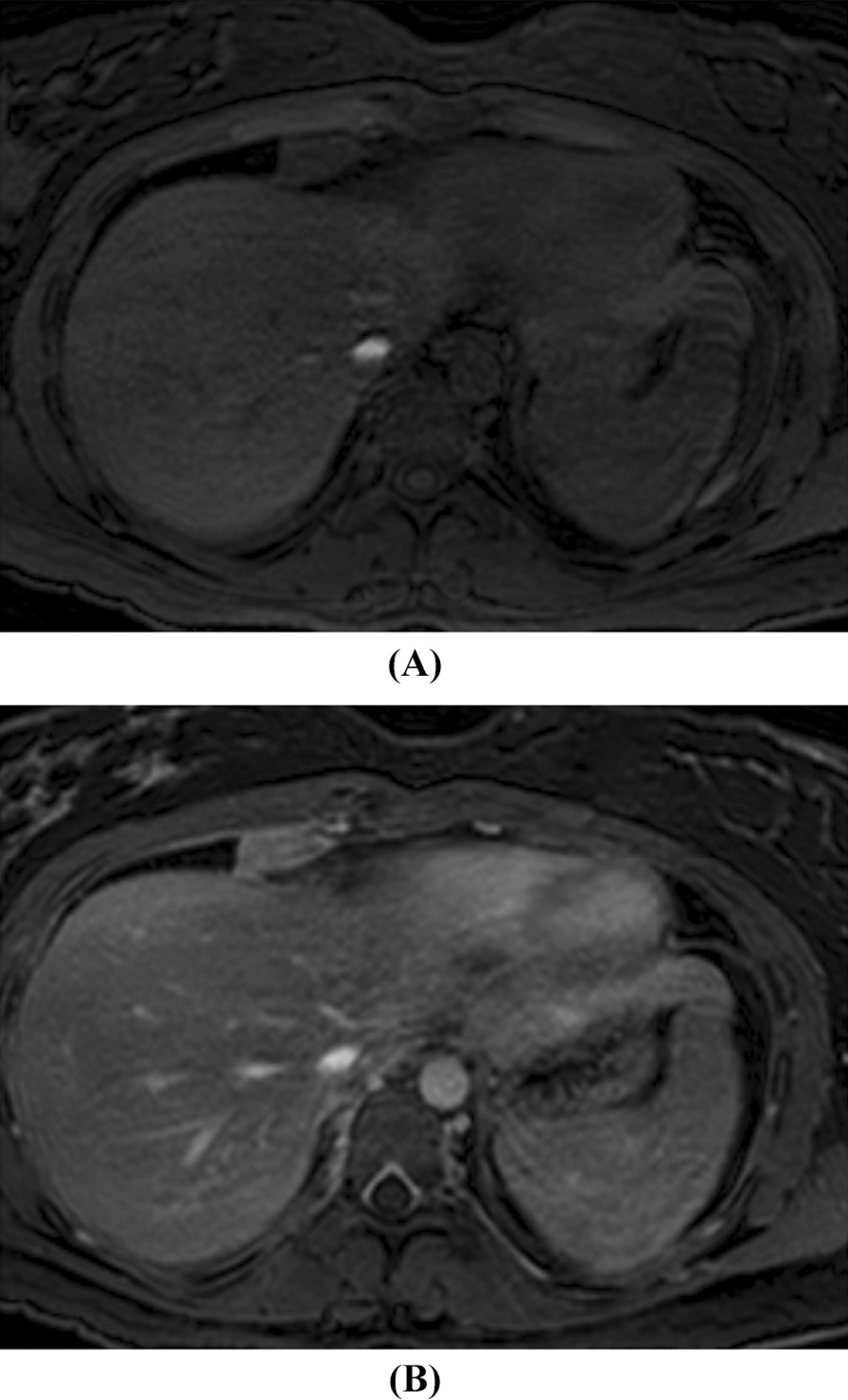
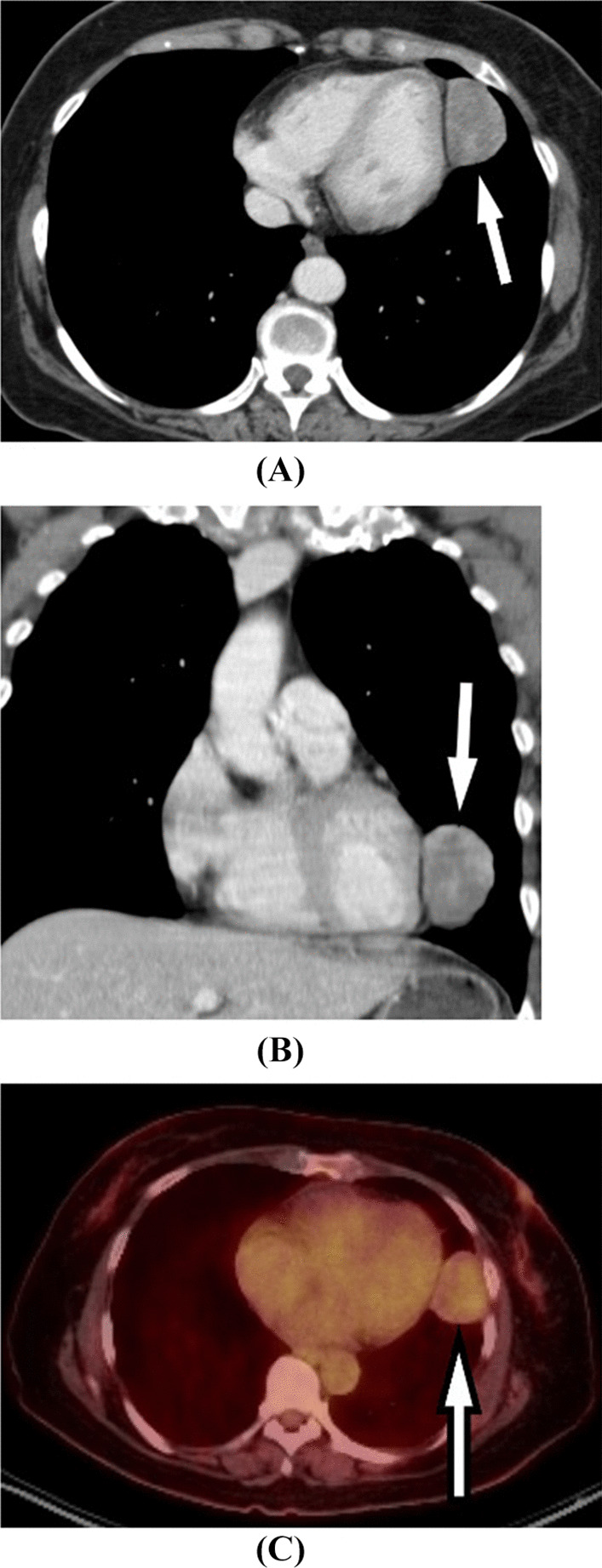
Solitary fibrous tumors (SFTs) are rare mesenchymal pleural neoplasms with an overall good prognosis and low recurrence rate if completely resected and if degree of differentiation is favorable. Within the last decade, advances in research have led to more reliable methods of differentiating SFTs from other soft tissue tumors. Historically, several markers were used to distinguish SFTs from similar tumors, but these markers had poor specificity. Recent evidence showed NAB2-STAT6 fusion gene to be a distinct feature of SFTs with 100% specificity and sensitivity. Surgical resection, with an emphasis on obtaining negative margins, is the mainstay of treatment for SFTs. Preoperative planning with detailed imaging is imperative to delineate the extent of disease and vascular supply. One important radiologic distinction to aid delineation of a pleural-based tumor compared to a pulmonary parenchymal-based tumor is the angle that the tumor forms with the chest wall, which is obtuse for a pleural-based tumor, and acute for tumors of the lung parenchyma. Often, preoperative tissue diagnosis is not available, and surgery is both diagnostic and curative. Intraoperatively, emphasis should be on complete resection with negative margins. SFTs are resected via several approaches: thoracotomy, sternotomy with the option of hemi-clamshell extension, video-assisted thoracoscopic surgery, and robotic approach, which is increasingly being used and is our preference. We recommend a minimally invasive approach for most lesions, and have resected SFTs of the pleura that are up to 12 cm with the robotic approach. However, the current literature often cites 5 cm as the cut off for an open thoracotomy. Nevertheless, even with larger tumors, a minimally invasive robotic approach is our preference and practice. For giant SFTs (> 20 cm), an open approach may be preferable. Multiple thoracotomies and rib resection may be required to gain adequate exposure and ensure complete resection in these tumors. However, it is noteworthy that most of these tumors have a soft consistency and thus, once bagged, can easily be removed minimally invasively, and thus minimally invasive approach should not be completely ruled out. Recurrence in SFTs usually results from incomplete resection and redo surgery may portend a favorable prognosis.
孤立性纤维瘤(SFT)是一种罕见的间叶性胸膜肿瘤,如果完全切除且分化程度良好,则总体预后良好,复发率低。在过去的十年中,研究的进展导致了更可靠的方法来区分 SFT 与其他软组织肿瘤。历史上,有几种标志物用于区分 SFT 与类似肿瘤,但这些标志物特异性较差。最近的证据表明,NAB2-STAT6 融合基因是 SFT 的一个独特特征,具有 100%的特异性和敏感性。强调获得阴性切缘的手术切除是 SFT 的主要治疗方法。详细的影像学术前规划对于描绘疾病的范围和血管供应至关重要。一个重要的影像学区别是,与肺实质肿瘤相比,胸膜肿瘤与胸壁形成的角度是钝角,而肺实质肿瘤的角度是锐角。通常,术前组织诊断不可用,手术既是诊断性的,也是治疗性的。术中应强调完全切除并获得阴性切缘。SFT 通过以下几种方法切除:开胸手术、胸骨切开术,可选半蛤壳式扩展、电视辅助胸腔镜手术和机器人手术,后者越来越多地被使用,也是我们的首选。我们建议大多数病变采用微创方法,并且已经使用机器人手术切除了最大达 12cm 的胸膜 SFT。然而,目前的文献经常引用 5cm 作为开胸手术的截止值。尽管如此,即使是更大的肿瘤,我们也更倾向于采用微创机器人手术。对于巨大的 SFT(>20cm),可能需要开放手术。这些肿瘤需要多次开胸和肋骨切除以获得足够的暴露并确保完全切除。然而,值得注意的是,大多数这些肿瘤质地柔软,因此一旦装袋,就可以很容易地微创取出,因此不应完全排除微创方法。SFT 的复发通常是由于不完全切除,如果再次手术可能预示着预后良好。