Department of Ophthalmology, University Medical Centre Regensburg, Franz-Josef-Strauß-Allee 11, 93053, Regensburg, Germany.
BMC Ophthalmol. 2023 Feb 24;23(1):75. doi: 10.1186/s12886-023-02823-6.
To investigate the incidence and clinical characteristics of unexplained visual loss in patients with fovea-sparing rhegmatogenous retinal detachment (RRD) during or after silicone oil (SO) tamponade.
The medical charts of all patients with macula-on RRDs, who underwent pars-plana-vitrectomy (ppV) with SO tamponade were retrospectively assessed regarding unexplained visual loss (UVL) of ≥ 3 Snellen lines and alterations on optical coherence tomography (OCT) during or after SO tamponade. The clinical data analysed included visual acuity, surgical parameters, OCT images, duration of SO tamponade and the time point of visual decline. Cases with re-detachment or secondary causes of visual loss such as SO emulsification, epiretinal membranes or macular edema were excluded.
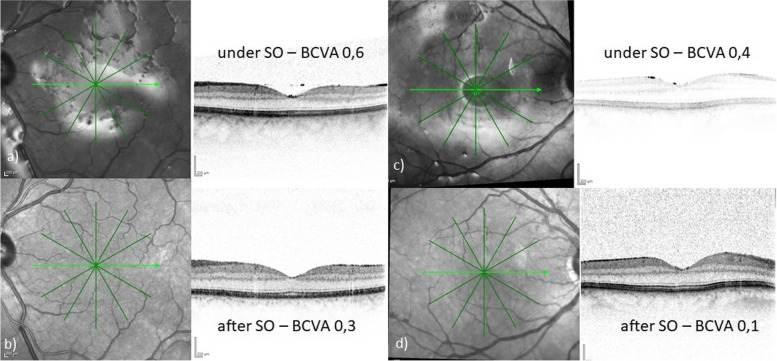
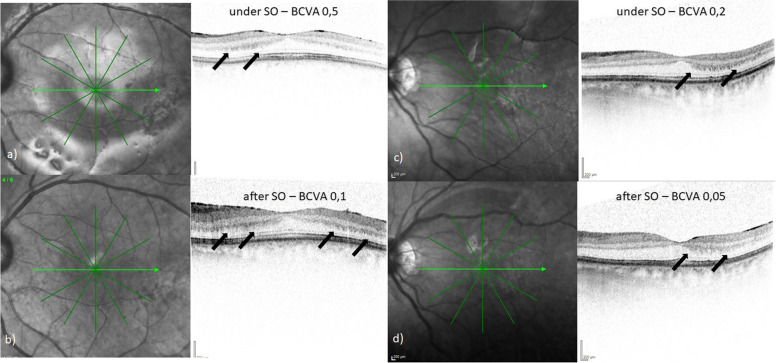
Over a 15-year-period, 22 cases with macula-on RRD, which had primarily been treated with ppV and SO tamponade, met the inclusion criteria. In most eyes (n = 20; 91%), the RRD was caused by a giant retinal tear (GRT). In 11 of these 22 cases (50%), best-corrected visual acuity (BCVA) had dropped by at least 3 lines for no apparent reason. In these 11 cases, mean preoperative logMAR BCVA was 0.2 (SD 0.13; range 0-0.5), equal to Snellen's VA of 0.63, and mean postoperative logMAR BCVA 1.0 (SD 0.24; range 0.5-1.3), equal to Snellen's VA of 0.10. Visual decline occurred about 12 weeks postoperatively (SD 6.2; range 3-20 ) and comprised 8 lines (SD 2.3; range -11 to -4). SO was removed on average 139 (SD 50.0; range 88-271) days after the first ppV. In 9 cases visual decline occurred while the SO was in-situ. In 2 patients, BCVA decline was noted 2 weeks after SO removal. In all eyes, preoperative central foveal thickness (CFT) was 254 μm (SD 24.2), which decreased to 224 μm (SD 29.6) during SO tamponade and increased to 247 μm (SD 29.2) after SO removal, irrespective of the presence of UVL. The mean follow-up time was 20 months (SD 30.6) after SO removal.
UVL after SO tamponade for macula-on RRD is more frequent than expected. The incidence in our case series was 50%. The mechanism of this phenomenon is still unknown. In general, vitreoretinal surgeons should thoroughly question the need for SO tamponade, inform their patients of possible UVL and remove SO as early as possible.
The study was approved by the local ethics committee on 6th of May 2022 (Ethikkommission der Universität Regensburg, Votum 22-2925-104) and was conducted in accordance with the ethical standards of the Declaration of Helsinki.
探讨硅油(SO)填充眼内期间或之后黄斑区保留的孔源性视网膜脱离(RRD)患者出现不明原因视力丧失(UVL)的发生率和临床特征。
回顾性分析所有接受过巩膜外垫压术联合 SO 填充的黄斑区 RRD 患者的病历资料,这些患者的最佳矫正视力(BCVA)下降≥3 行,且在 SO 填充期间或之后的光学相干断层扫描(OCT)上出现改变。分析的临床数据包括视力、手术参数、OCT 图像、SO 填充时间和视力下降时间。排除再次脱离或 SO 乳化、视网膜前膜或黄斑水肿等继发性视力丧失的病例。
在 15 年的时间里,共有 22 例黄斑区 RRD 患者符合纳入标准,这些患者最初接受了巩膜外垫压术联合 SO 填充。在大多数眼(n=20;91%)中,RRD 是由巨大裂孔(GRT)引起的。在这 22 例患者中,有 11 例(50%)的 BCVA 不明原因下降至少 3 行。在这 11 例患者中,术前平均 logMAR BCVA 为 0.2(SD 0.13;范围 0-0.5),相当于 Snellen 视力的 0.63,术后平均 logMAR BCVA 为 1.0(SD 0.24;范围 0.5-1.3),相当于 Snellen 视力的 0.10。视力下降发生在术后约 12 周(SD 6.2;范围 3-20),下降 8 行(SD 2.3;范围-11 至-4)。SO 平均在首次巩膜外垫压术后 139 天(SD 50.0;范围 88-271)被移除。在 9 例患者中,SO 在位时出现视力下降。在 2 例患者中,SO 移除后 2 周出现 BCVA 下降。所有眼的术前中央视网膜厚度(CFT)为 254μm(SD 24.2),SO 填充期间降至 224μm(SD 29.6),SO 移除后增加至 247μm(SD 29.2),与 UVL 的存在无关。SO 移除后的平均随访时间为 20 个月(SD 30.6)。
黄斑区 RRD 患者在 SO 填充后出现 UVL 的频率高于预期。在我们的病例系列中,这一发生率为 50%。这种现象的机制仍不清楚。一般来说,玻璃体视网膜外科医生应该彻底询问 SO 填充的必要性,告知患者可能出现的 UVL,并尽早移除 SO。
注:此译文仅供参考,具体内容请以英文原文为准。