Torres-Arrese Marta, Mata-Martínez Arantzazu, Luordo-Tedesco Davide, García-Casasola Gonzalo, Alonso-González Rodrigo, Montero-Hernández Esther, Cobo-Marcos Marta, Sánchez-Sauce Beatriz, Cuervas-Mons Valentín, Tung-Chen Yale
Department of Emergency Medicine, Hospital Universitario Fundación de Alcorcón, Calle Budapest 1, 28922 Alcorcón, Spain.
Department of Emergency Medicine, Hospital Universitario Infanta Cristina, Avenida 9 de Junio 2, 28981 Parla, Spain.
J Clin Med. 2023 Feb 6;12(4):1281. doi: 10.3390/jcm12041281.
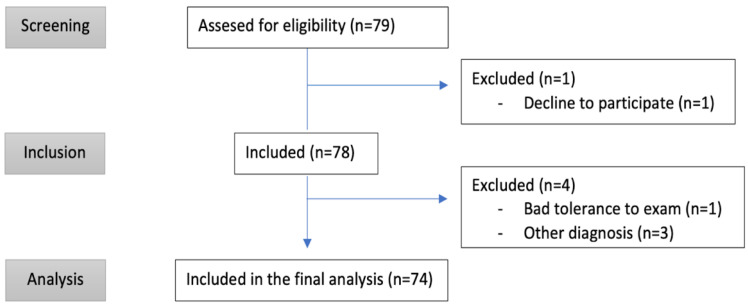
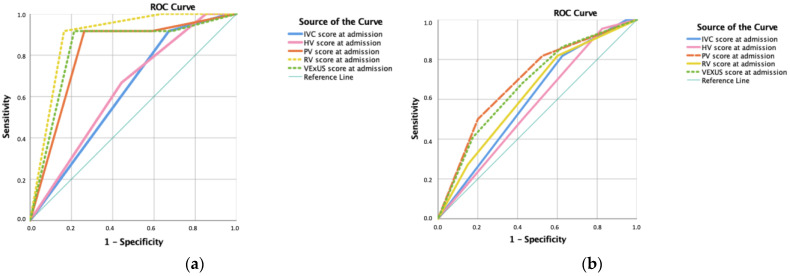
Mortality and re-admission rates for decompensated acute heart failure (AHF) is increasing overall and risk stratification might be challenging. We sought to evaluate the prognostic role of systemic venous ultrasonography in patients hospitalized for AHF. We prospectively recruited 74 AHF patients with a NT-proBNP level above 500 pg/mL. Then, multi-organ ultrasound assessments (lung, inferior vena cava (IVC), pulsed-wave Doppler (PW-Doppler) of hepatic, portal, intra-renal and femoral veins) were performed at admission, discharge, and follow-up (for 90 days). We also calculated the Venous Excess Ultrasound System (VExUS), a new score of systemic congestion based on IVC dilatation and pulsed-wave Doppler morphology of hepatic, portal and intra-renal veins. An intra-renal monophasic pattern (area under the curve (AUC) 0.923, sensitivity (Sn) 90%, specificity (Sp) 81%, positive predictive value (PPV) 43%, and negative predictive value (NPV) 98%), a portal pulsatility > 50% (AUC 0.749, Sn 80%, Sp 69%, PPV 30%, NPV 96%) and a VExUS score of 3 corresponding to severe congestion (AUC 0.885, Sn 80%, Sp 75%, PPV 33%, and NPV 96%) predicted death during hospitalization. An IVC above 2 cm (AUC 0.758, Sn 93.l% and Sp 58.3) and the presence of an intra-renal monophasic pattern (AUC 0. 834, sensitivity 0.917, specificity 67.4%) in the follow-up visit predicted AHF-related re-admission. Additional scans during hospitalization or the calculation of a VExUS score probably adds unnecessary complexity to the assessment of AHF patients. In conclusion, VExUS score does not contribute to the guidance of therapy or the prediction of complications, compared with the presence of an IVC greater than 2 cm, a venous monophasic intra-renal pattern or a pulsatility > 50% of the portal vein in AHF patients. Early and multidisciplinary follow-up visits remain necessary for the improvement of the prognosis of this highly prevalent disease.
失代偿性急性心力衰竭(AHF)的死亡率和再入院率总体呈上升趋势,风险分层可能具有挑战性。我们旨在评估全身静脉超声检查在因AHF住院患者中的预后作用。我们前瞻性招募了74例NT-proBNP水平高于500 pg/mL的AHF患者。然后,在入院、出院及随访(90天)时进行多器官超声评估(肺部、下腔静脉(IVC)、肝静脉、门静脉、肾内静脉和股静脉的脉冲波多普勒(PW-Doppler))。我们还计算了静脉超声系统(VExUS),这是一种基于IVC扩张以及肝静脉、门静脉和肾内静脉脉冲波多普勒形态的全身充血新评分。肾内单相模式(曲线下面积(AUC)0.923,敏感性(Sn)90%,特异性(Sp)81%,阳性预测值(PPV)43%,阴性预测值(NPV)98%)、门静脉搏动性>50%(AUC 0.749,Sn 80%,Sp 69%,PPV 30%,NPV 96%)以及VExUS评分为3对应严重充血(AUC 0.885,Sn 80%,Sp 75%,PPV 33%,NPV 96%)可预测住院期间死亡。随访时IVC大于2 cm(AUC 0.758,Sn 93.1%,Sp 58.3)以及存在肾内单相模式(AUC 0.834,敏感性0.917,特异性67.4%)可预测与AHF相关的再入院。住院期间进行额外扫描或计算VExUS评分可能会给AHF患者的评估增加不必要的复杂性。总之,与AHF患者中IVC大于2 cm、肾内静脉单相模式或门静脉搏动性>50%相比,VExUS评分对治疗指导或并发症预测并无帮助。早期多学科随访对于改善这种高流行疾病的预后仍然必要。