Phoenix Epidemiology and Clinical Research Branch, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Phoenix, AZ, USA.
Nuffield Department of Medicine, University of Oxford, Oxford, UK.
Diabetologia. 2023 May;66(5):847-860. doi: 10.1007/s00125-023-05870-2. Epub 2023 Mar 2.
AIMS/HYPOTHESIS: There is limited information on how polygenic scores (PSs), based on variants from genome-wide association studies (GWASs) of type 2 diabetes, add to clinical variables in predicting type 2 diabetes incidence, particularly in non-European-ancestry populations.
For participants in a longitudinal study in an Indigenous population from the Southwestern USA with high type 2 diabetes prevalence, we analysed ten constructions of PS using publicly available GWAS summary statistics. Type 2 diabetes incidence was examined in three cohorts of individuals without diabetes at baseline. The adult cohort, 2333 participants followed from age ≥20 years, had 640 type 2 diabetes cases. The youth cohort included 2229 participants followed from age 5-19 years (228 cases). The birth cohort included 2894 participants followed from birth (438 cases). We assessed contributions of PSs and clinical variables in predicting type 2 diabetes incidence.
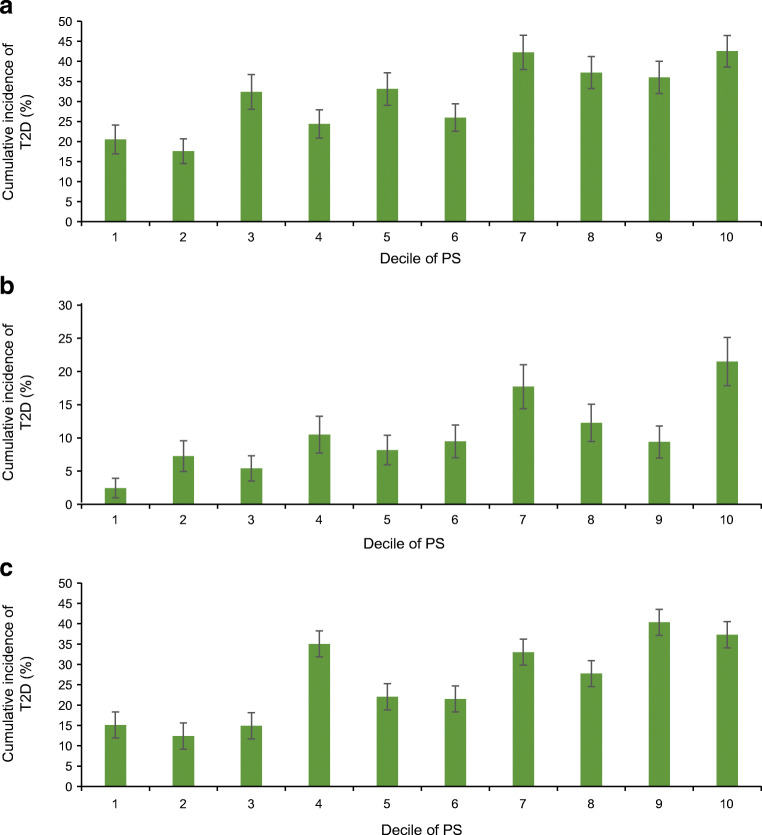
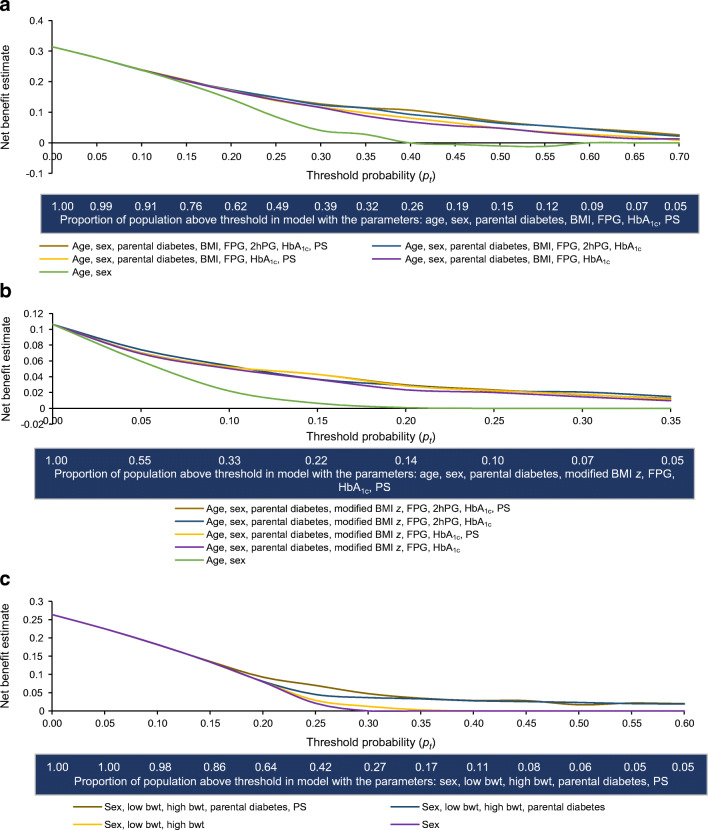
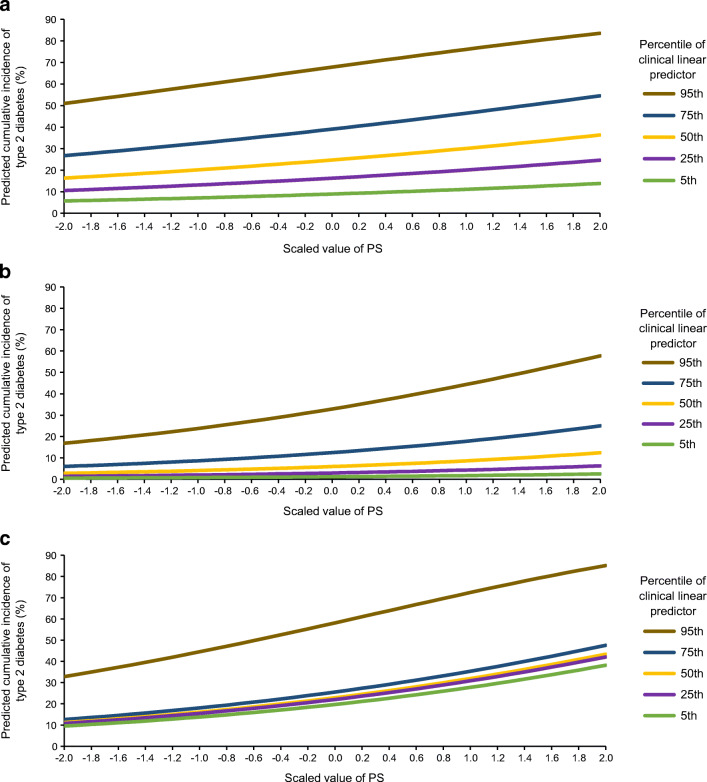
Of the ten PS constructions, a PS using 293 genome-wide significant variants from a large type 2 diabetes GWAS meta-analysis in European-ancestry populations performed best. In the adult cohort, the AUC of the receiver operating characteristic curve for clinical variables for prediction of incident type 2 diabetes was 0.728; with the PS, 0.735. The PS's HR was 1.27 per SD (p=1.6 × 10; 95% CI 1.17, 1.38). In youth, corresponding AUCs were 0.805 and 0.812, with HR 1.49 (p=4.3 × 10; 95% CI 1.29, 1.72). In the birth cohort, AUCs were 0.614 and 0.685, with HR 1.48 (p=2.8 × 10; 95% CI 1.35, 1.63). To further assess the potential impact of including PS for assessing individual risk, net reclassification improvement (NRI) was calculated: NRI for the PS was 0.270, 0.268 and 0.362 for adult, youth and birth cohorts, respectively. For comparison, NRI for HbA was 0.267 and 0.173 for adult and youth cohorts, respectively. In decision curve analyses across all cohorts, the net benefit of including the PS in addition to clinical variables was most pronounced at moderately stringent threshold probability values for instituting a preventive intervention.
CONCLUSIONS/INTERPRETATION: This study demonstrates that a European-derived PS contributes significantly to prediction of type 2 diabetes incidence in addition to information provided by clinical variables in this Indigenous study population. Discriminatory power of the PS was similar to that of other commonly measured clinical variables (e.g. HbA). Including type 2 diabetes PS in addition to clinical variables may be clinically beneficial for identifying individuals at higher risk for the disease, especially at younger ages.
目的/假设:基于 2 型糖尿病全基因组关联研究(GWAS)的变异体的多基因评分(PSs)在预测 2 型糖尿病发病方面如何与临床变量相结合,这方面的信息有限,特别是在非欧洲血统人群中。
对于来自美国西南部具有高 2 型糖尿病患病率的土著人群的纵向研究中的参与者,我们使用公开的 GWAS 汇总统计数据分析了十种 PS 结构。在基线时没有糖尿病的三个个体队列中检查了 2 型糖尿病的发病率。成人队列包括 2333 名年龄≥20 岁的参与者,有 640 例 2 型糖尿病病例。青年队列包括 2229 名年龄在 5-19 岁的参与者(228 例)。出生队列包括 2894 名从出生开始随访的参与者(438 例)。我们评估了 PSs 和临床变量在预测 2 型糖尿病发病中的作用。
在十种 PS 结构中,使用来自大型欧洲血统 2 型糖尿病 GWAS 荟萃分析的 293 个全基因组显著变异体的 PS 表现最佳。在成人队列中,预测事件性 2 型糖尿病的临床变量的受试者工作特征曲线的 AUC 为 0.728;PS 为 0.735。PS 的 HR 为每 SD 1.27(p=1.6×10;95%CI 1.17,1.38)。在年轻人中,相应的 AUC 分别为 0.805 和 0.812,HR 为 1.49(p=4.3×10;95%CI 1.29,1.72)。在出生队列中,AUC 分别为 0.614 和 0.685,HR 为 1.48(p=2.8×10;95%CI 1.35,1.63)。为了进一步评估纳入 PS 评估个体风险的潜在影响,计算了净重新分类改善(NRI):PS 的 NRI 分别为成人、青年和出生队列的 0.270、0.268 和 0.362。相比之下,成人和青年队列中 HbA 的 NRI 分别为 0.267 和 0.173。在所有队列的决策曲线分析中,在中度严格的预防性干预起始概率值下,加入 PS 除临床变量外的净获益最为明显。
结论/解释:本研究表明,在这个土著人群中,来自欧洲的 PS 除了提供临床变量信息外,还显著有助于预测 2 型糖尿病的发病。PS 的判别能力与其他常用的临床测量指标(如 HbA)相似。除了临床变量外,还纳入 2 型糖尿病 PS 可能对识别疾病风险较高的个体具有临床益处,尤其是在较年轻时。