Klimis Harry, Pinthus Jehonathan H, Aghel Nazanin, Duceppe Emmanuelle, Fradet Vincent, Brown Ian, Siemens D Robert, Shayegan Bobby, Klotz Laurence, Luke Patrick P, Niazi Tamim, Lavallee Luke T, Mousavi Negareh, Hamilton Robert J, Chin Joseph L, Gopaul Darin, Violette Philippe D, Davis Margot K, Hanna Nawar, Sabbagh Robert, Ben Zadok Osnat Itzhaki, Hajjar Ludhmila Abrahão, Kann Ariel Galapo, Mian Rajibul, Rangarajan Sumathy, Huei Ng Kelvin Kuan, Iakobishvili Zaza, Selvanayagam Joseph B, Avezum Alvaro, Leong Darryl P
Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, Ontario, Canada.
Department of Surgery, McMaster University, Hamilton, Ontario, Canada.
JACC CardioOncol. 2023 Jan 17;5(1):70-81. doi: 10.1016/j.jaccao.2022.09.008. eCollection 2023 Feb.
Cardiovascular disease (CVD) incidence is higher in men with prostate cancer (PC) than without.
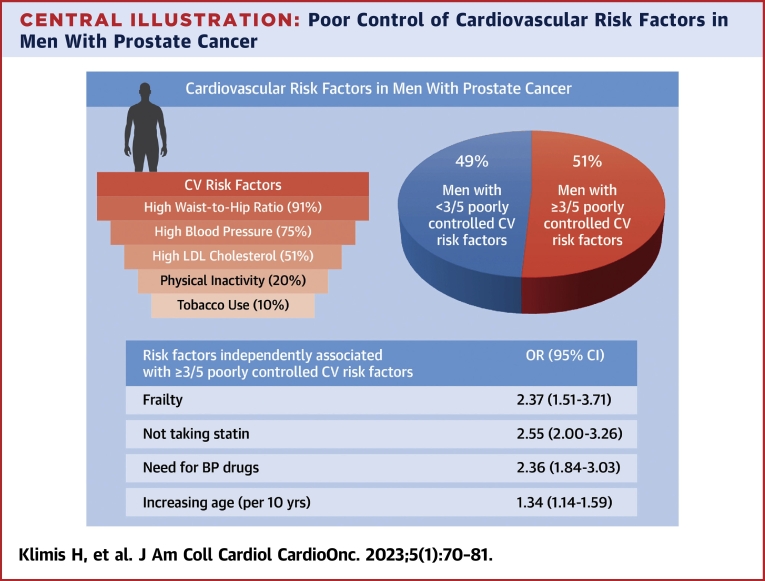
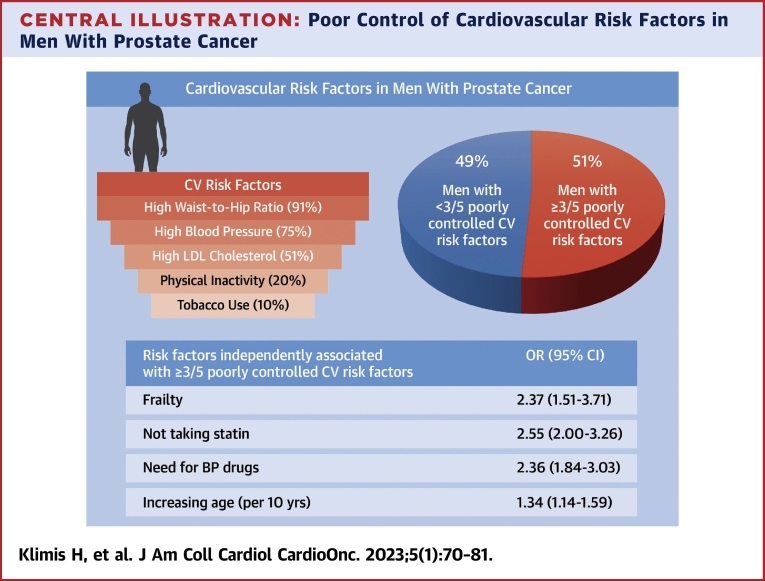
We describe the rate and correlates of poor cardiovascular risk factor control among men with PC.
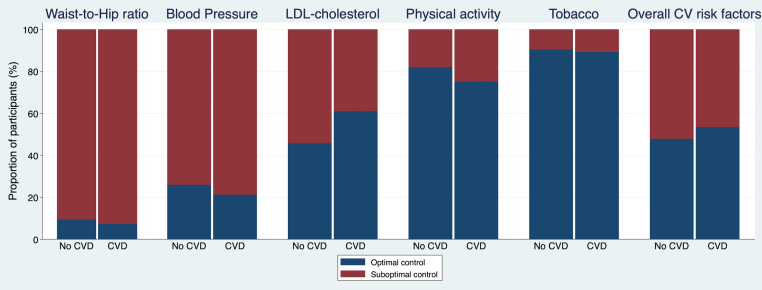
We prospectively characterized 2,811 consecutive men (mean age 68 ± 8 years) with PC from 24 sites in Canada, Israel, Brazil, and Australia. We defined poor overall risk factor control as ≥3 of the following: suboptimal low-density lipoprotein cholesterol (>2 mmol/L if Framingham Risk Score [FRS] ≥15 and ≥3.5 mmol/L if FRS <15), current smoker, physical inactivity (<600 MET min/wk), suboptimal blood pressure (BP) (≥140/90 mm Hg if no other risk factors, systolic BP 120 mm Hg if known CVD or FRS ≥15, and ≥130/80 mm Hg if diabetic), and waist:hip ratio >0.9.
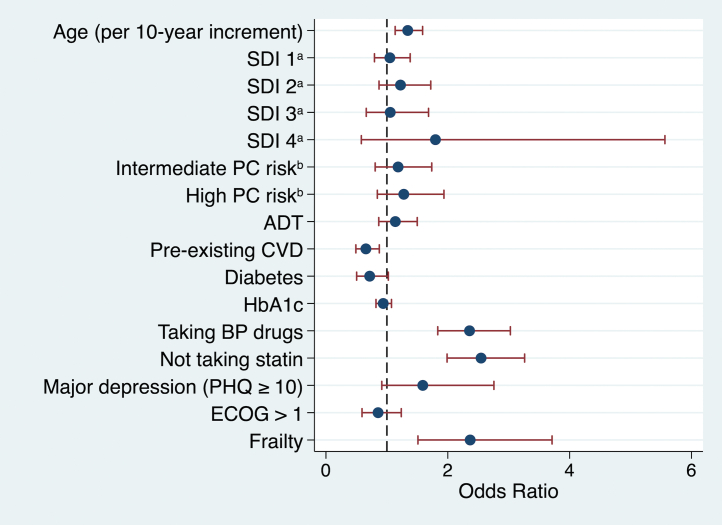
Among participants (9% with metastatic PC and 23% with pre-existing CVD), 99% had ≥1 uncontrolled cardiovascular risk factor, and 51% had poor overall risk factor control. Not taking a statin (odds ratio [OR]: 2.55; 95% CI: 2.00-3.26), physical frailty (OR: 2.37; 95% CI: 1.51-3.71), need for BP drugs (OR: 2.36; 95% CI: 1.84-3.03), and age (OR per 10-year increase: 1.34; 95% CI: 1.14-1.59) were associated with poor overall risk factor control after adjustment for education, PC characteristics, androgen deprivation therapy, depression, and Eastern Cooperative Oncology Group functional status.
Poor control of modifiable cardiovascular risk factors is common in men with PC, highlighting the large gap in care and the need for improved interventions to optimize cardiovascular risk management in this population.
前列腺癌(PC)男性的心血管疾病(CVD)发病率高于无前列腺癌的男性。
我们描述了PC男性中不良心血管危险因素控制的发生率及其相关因素。
我们前瞻性地对来自加拿大、以色列、巴西和澳大利亚24个地点的2811名连续入选的PC男性(平均年龄68±8岁)进行了特征分析。我们将总体危险因素控制不佳定义为符合以下≥3项情况:低密度脂蛋白胆固醇未达最佳水平(如果弗雷明汉风险评分[FRS]≥15,则>2 mmol/L;如果FRS<15,则≥3.5 mmol/L)、当前吸烟者、身体活动不足(<600 MET·分钟/周)、血压(BP)未达最佳水平(如果无其他危险因素,则≥140/90 mmHg;如果已知患有CVD或FRS≥15,则收缩压≥120 mmHg;如果患有糖尿病,则≥130/80 mmHg),以及腰臀比>0.9。
在参与者中(9%患有转移性PC,23%患有既往CVD),99%有≥1项未得到控制的心血管危险因素,51%总体危险因素控制不佳。在对教育程度、PC特征、雄激素剥夺治疗、抑郁和东部肿瘤协作组功能状态进行调整后,未服用他汀类药物(比值比[OR]:2.55;95%置信区间[CI]:2.00 - 3.26)、身体虚弱(OR:2.37;95% CI:1.51 - 3.71)、需要服用降压药物(OR:2.36;95% CI:1.84 - 3.03)和年龄(每增加10岁的OR:1.34;95% CI:1.14 - 1.59)与总体危险因素控制不佳相关。
可改变的心血管危险因素控制不佳在PC男性中很常见,这突出了护理方面的巨大差距,以及需要改进干预措施以优化该人群的心血管风险管理。