Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Hamburg Center for Health Economics, Martinistraße 52 Building W37, 20246 Hamburg, Germany.
Department of Cardiology, University Heart and Vascular Center Hamburg-Eppendorf, Martinistraße 52, Hamburg 20246, Germany.
Europace. 2023 May 19;25(5). doi: 10.1093/europace/euad051.
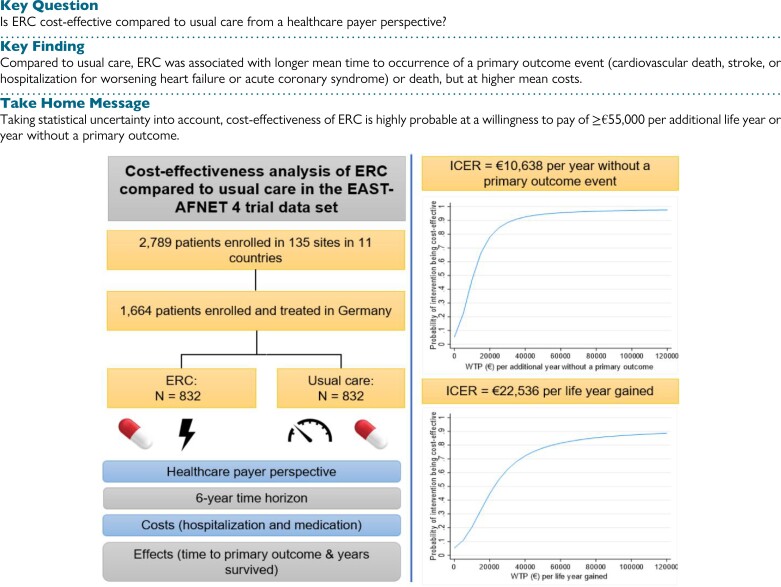
The randomized, controlled EAST-AFNET 4 trial showed that early rhythm control (ERC) reduces the rate of a composite primary outcome (cardiovascular death, stroke, or hospitalization for worsening heart failure or acute coronary syndrome) by ∼20%. The current study examined the cost-effectiveness of ERC compared to usual care.
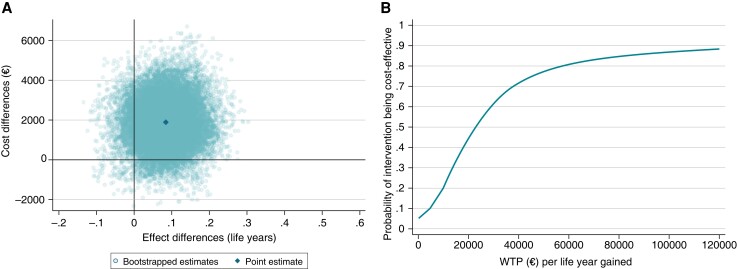
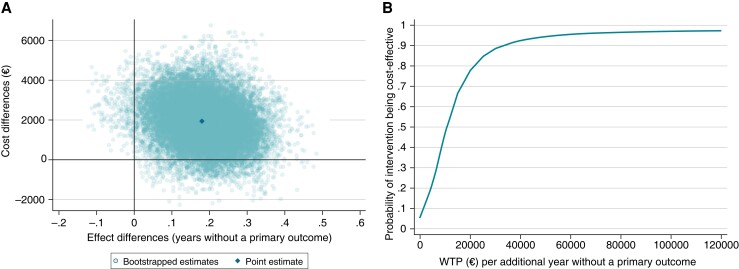
This within-trial cost-effectiveness analysis was based on data from the German subsample of the EAST-AFNET 4 trial (n = 1664/2789 patients). Over a 6-year time horizon and from a healthcare payer's perspective, ERC was compared to usual care regarding costs (hospitalization and medication) and effects (time to primary outcome; years survived). Incremental cost-effectiveness ratios (ICERs) were calculated. Cost-effectiveness acceptability curves were constructed to visualize uncertainty. Early rhythm control was associated with higher costs [+€1924, 95% CI (-€399, €4246)], resulting in ICERs of €10 638 per additional year without a primary outcome and €22 536 per life year gained. The probability of ERC being cost-effective compared to usual care was ≥95% or ≥80% at a willingness-to-pay value of ≥€55 000 per additional year without a primary outcome or life year gained, respectively.
From a German healthcare payer's perspective, health benefits of ERC may come at reasonable costs as indicated by the ICER point estimates. Taking statistical uncertainty into account, cost-effectiveness of ERC is highly probable at a willingness-to-pay value of ≥€55 000 per additional life year or year without a primary outcome. Future studies examining the cost-effectiveness of ERC in other countries, subgroups with higher benefit from rhythm control therapy, or cost-effectiveness of different modes of ERC are warranted.
随机对照 EAST-AFNET 4 试验表明,早期节律控制(ERC)可使复合主要结局(心血管死亡、卒中和因心力衰竭恶化或急性冠状动脉综合征而住院)的发生率降低约 20%。本研究旨在探讨 ERC 相对于常规治疗的成本效益。
本项基于 EAST-AFNET 4 试验德国亚组数据的试验内成本效益分析(n=1664/2789 例患者)。在 6 年的时间内,从医疗保健支付者的角度出发,将 ERC 与常规治疗进行了比较,比较内容包括成本(住院和药物治疗)和效果(主要结局发生时间;年生存率)。计算了增量成本效益比(ICER)。构建成本效益接受曲线以可视化不确定性。早期节律控制与较高的成本相关[+€1924,95%置信区间(-€399,€4246)],导致每增加一年无主要结局的 ICER 为€10638 元,每增加一年生存的 ICER 为€22536 元。与常规治疗相比,ERC 的成本效益比≥95%或≥80%的概率≥€55000 元,每增加一年无主要结局或每增加一年生存的意愿支付价值分别为€55000 元或 €22536 元。
从德国医疗保健支付者的角度来看,ERC 的健康获益可能在合理的成本范围内,这一点可以从 ICER 点估计值看出。考虑到统计不确定性,在每增加一年生存或无主要结局的意愿支付价值≥€55000 元时,ERC 的成本效益极有可能。未来的研究需要在其他国家、节律控制治疗获益更高的亚组以及不同 ERC 模式的成本效益方面进行研究。