S.C. Medicina d'Urgenza U (MECAU), Ospedale Molinette, A.O.U. Città della Salute e della Scienza, 10126 Torino, Italy.
Dipartimento di Scienze Mediche, Università degli Studi di Torino, 10126 Torino, Italy.
Medicina (Kaunas). 2023 Mar 10;59(3):548. doi: 10.3390/medicina59030548.
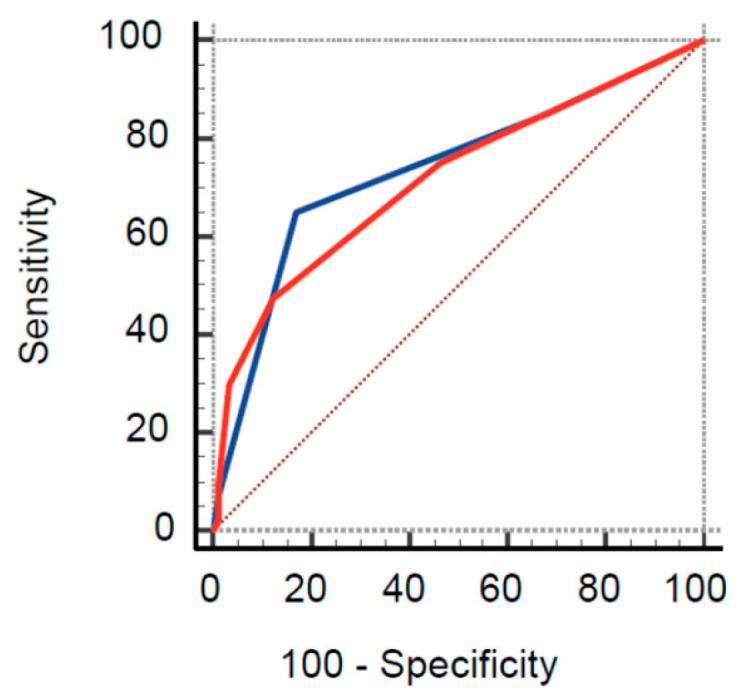
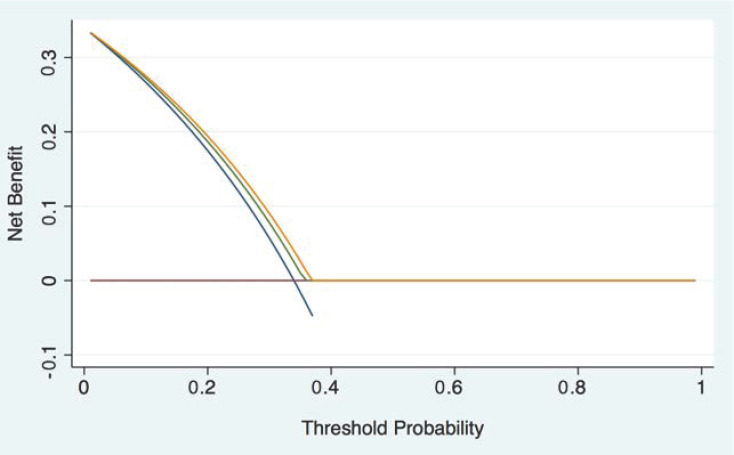
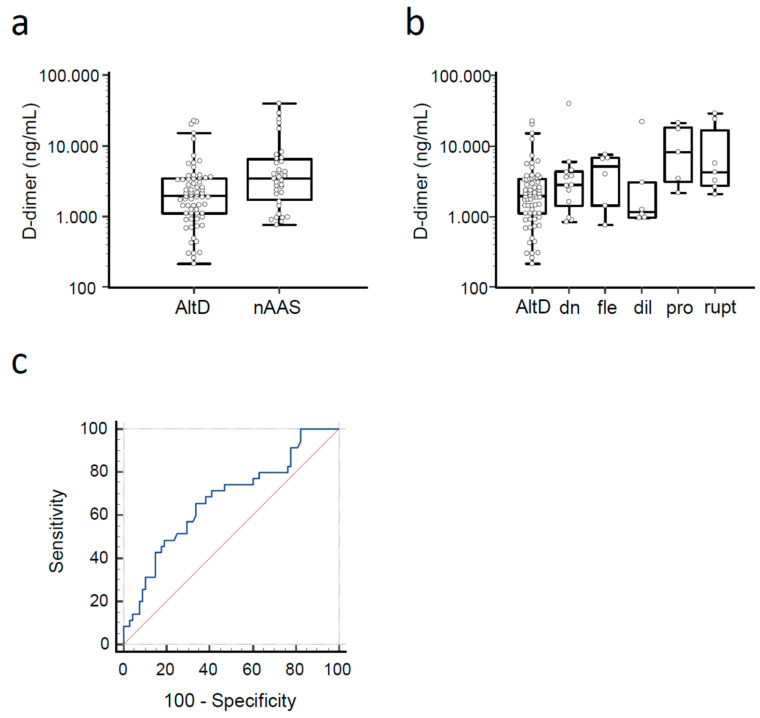
. Acute aortic syndromes (AASs) are emergencies burdened by high morbidity and mortality. Guideline-recommended diagnostic workup is based on pre-test probability assessment (PPA) and d-dimer testing. However, the performance of PPA and d-dimer has never been studied in individuals with previous AAS (pAAS), which represent a challenging population. . We analyzed a registry of patients with pAAS evaluated in two Emergency Departments (EDs) for suspected novel AAS (nAAS). Enrolment criteria were history of pAAS and the presence of truncal pain, syncope or perfusion deficit. All patients underwent advanced imaging. Clinical data were registered prospectively and PPA was performed by applying the aortic dissection detection (ADD) and an aorta simplified (AORTAs) score. . A total of 128 patients were enrolled, including 77 patients with previous Stanford type A aortic dissection and 45 patients with previous Stanford type B aortic dissection. The final diagnosis was nAAS in 40 (31%) patients. Clinical variables associated with nAAS were: aortic valve disease, thoracic aortic aneurysm, severe pain, sudden pain, ripping/tearing pain and hypotension/shock. ADD score ≥ 2 had a sensitivity of 65% and a specificity of 83% for nAAS; AORTAs score ≥ 2 had a sensitivity of 48% and a specificity of 88%. d-dimer (cutoff ≥ 500 ng/mL or age-adjusted cutoff) had a sensitivity of 97% and a specificity of 13%/14.7%, for diagnosis of nAAS. Patients that were candidates for guideline-compliant PPA/d-dimer integrated rule-out were: 5 (4.9%) with ADD ≤ 1/d-dimer and 8 (7.8%) with AORTAs ≤ 1/d-dimer < age-adjusted cutoff. None of them had a nAAS. . Patients with pAAS evaluated in the ED for red-flag symptoms showed intermediate-to-high pre-test probability of nAAS. The ADD score had lower sensitivity and specificity than in unselected patients. d-dimer, alone and integrated with PPA, was highly sensitive for nAAS, but very unspecific. PPA/d-dimer integrated strategies are unlikely to significantly reduce the number of patients with pAAS undergoing advanced imaging.
急性主动脉综合征(AAS)是一种发病率和死亡率都很高的急症。指南推荐的诊断方法基于术前概率评估(PPA)和 D-二聚体检测。然而,PPA 和 D-二聚体在有既往 AAS(pAAS)病史的患者中的表现从未被研究过,这些患者代表了一个具有挑战性的人群。我们分析了在两个急诊部(ED)就诊的疑似新发 AAS(nAAS)患者的 pAAS 登记数据。入组标准为有 pAAS 病史和躯干疼痛、晕厥或灌注不足。所有患者均接受了高级影像学检查。临床数据前瞻性登记,应用主动脉夹层检测(ADD)和简化主动脉评分(AORTAs)进行 PPA。共纳入 128 例患者,其中 77 例为既往 Stanford 型 A 型主动脉夹层,45 例为既往 Stanford 型 B 型主动脉夹层。最终诊断为 40 例(31%)nAAS。与 nAAS 相关的临床变量为:主动脉瓣疾病、胸主动脉瘤、剧烈疼痛、突发疼痛、撕裂样疼痛和低血压/休克。ADD 评分≥2 时,nAAS 的敏感性为 65%,特异性为 83%;AORTAs 评分≥2 时,敏感性为 48%,特异性为 88%。D-二聚体(截断值≥500ng/ml 或年龄校正截断值)对 nAAS 的诊断敏感性为 97%,特异性为 13%/14.7%。符合指南的 PPA/D-二聚体综合排除标准的患者为:ADD≤1/D-二聚体且<年龄校正截断值的患者 5 例(4.9%),AORTAs≤1/D-二聚体<年龄校正截断值的患者 8 例(7.8%)。他们均未发生 nAAS。在 ED 就诊的有红色警报症状的 pAAS 患者,新发 AAS 的术前概率为中高度。ADD 评分的敏感性和特异性均低于未选择的患者。D-二聚体单独或与 PPA 联合应用对 nAAS 高度敏感,但特异性很低。PPA/D-二聚体综合策略不太可能显著减少接受高级影像学检查的 pAAS 患者数量。