Baral Ranju, Higgins Deborah, Regan Katie, Pecenka Clint
Center for Vaccine Innovation and Access, Program for Appropriate Technology in Health, Seattle, Washington, USA
Center for Vaccine Innovation and Access, Program for Appropriate Technology in Health, Seattle, Washington, USA.
BMJ Open. 2021 Apr 24;11(4):e046563. doi: 10.1136/bmjopen-2020-046563.
Interventions to prevent childhood respiratory syncytial virus (RSV) disease are limited and costly. New interventions are in advanced stages of development and could be available soon. This study aims to evaluate the potential impact and cost-effectiveness of two interventions to prevent childhood RSV-a maternal vaccine and a monoclonal antibody (mAb).
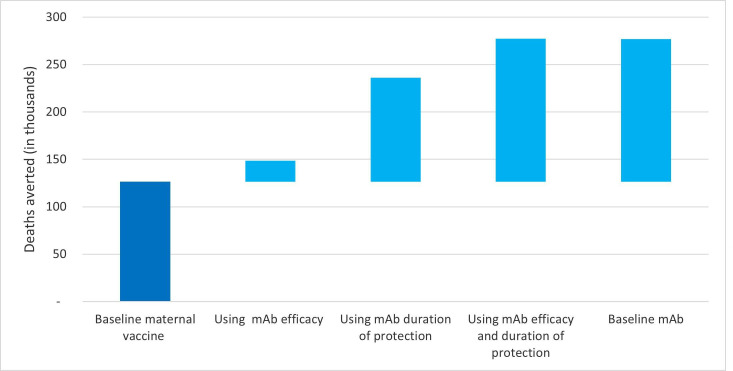
Using a static population-based cohort model, we evaluate impact and cost-effectiveness of RSV interventions, from a health systems perspective. The assumed baseline efficacy and duration of protection were higher for the mAb (60%-70% efficacy, protection 6 months) compared with the maternal vaccine (40%-60% efficacy, protection 3 months). Both interventions were evaluated at US$3 and US$5 per dose for Gavi and non-Gavi countries, respectively. A range of input values were considered to explore uncertainty.
131 low-income and middle-income countries.
Pregnant women and live birth cohorts.
Maternal vaccine given to pregnant women and mAb given to young infants.
Disability-adjusted life years averted, severe case averted, deaths averted, incremental cost effectiveness ratios.
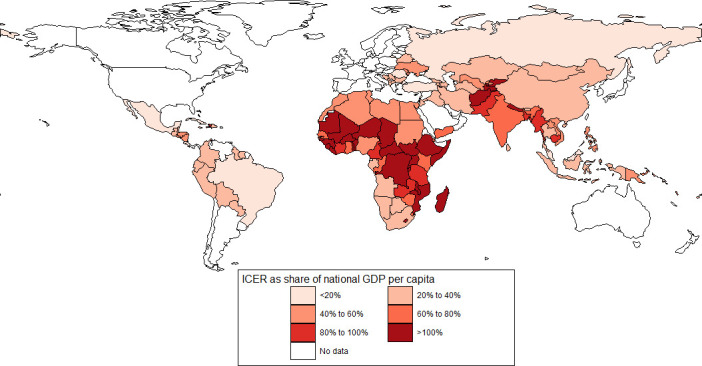
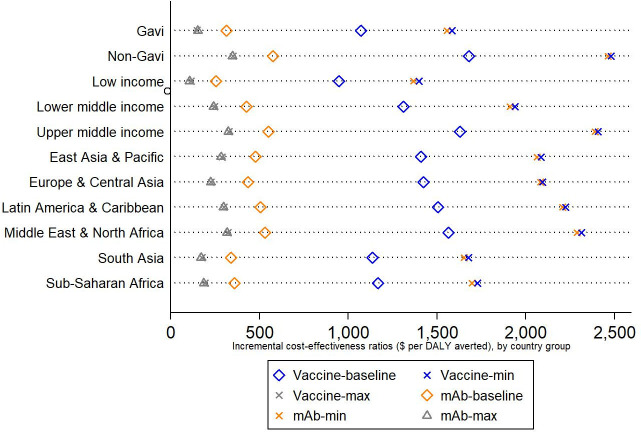
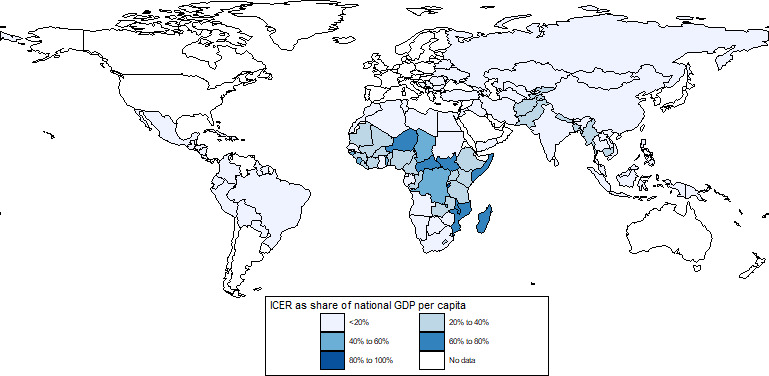
Under baseline assumptions, maternal vaccine and mAbs were projected to avert 25% and 55% of RSV-related deaths among infants younger than 6 months of age, respectively. The average incremental cost-effectiveness ratio per disability-adjusted life year averted was US$1342 (range US$800-US$1866) for maternal RSV vaccine and US$431 (range US$167-US$692) for mAbs. At a 50% gross domestic product per capita threshold, maternal vaccine and mAbs were cost-effective in 60 and 118 countries, respectively.
Both interventions are projected to be impactful and cost-effective in many countries, a finding that would be enhanced if country-specific Gavi cofinancing to eligible countries were included. mAbs, with assumed higher efficacy and duration of protection, are expected to be more cost-effective than RSV maternal vaccines at similar prices. Final product characteristics will influence this finding.
预防儿童呼吸道合胞病毒(RSV)疾病的干预措施有限且成本高昂。新的干预措施正处于研发后期,可能很快就能投入使用。本研究旨在评估两种预防儿童RSV的干预措施——一种母体疫苗和一种单克隆抗体(mAb)——的潜在影响和成本效益。
我们使用基于静态人群的队列模型,从卫生系统的角度评估RSV干预措施的影响和成本效益。假设单克隆抗体的基线疗效和保护持续时间(疗效60%-70%,保护6个月)高于母体疫苗(疗效40%-60%,保护3个月)。对于全球疫苗免疫联盟(Gavi)国家和非Gavi国家,两种干预措施每剂的评估价格分别为3美元和5美元。考虑了一系列输入值以探索不确定性。
131个低收入和中等收入国家。
孕妇和活产队列。
给孕妇接种母体疫苗,给幼儿注射单克隆抗体。
避免的伤残调整生命年、避免的严重病例、避免的死亡、增量成本效益比。
在基线假设下,预计母体疫苗和单克隆抗体分别可避免6个月以下婴儿中25%和55%的RSV相关死亡。每避免一个伤残调整生命年,母体RSV疫苗的平均增量成本效益比为1342美元(范围800美元-1866美元),单克隆抗体为431美元(范围167美元-692美元)。在人均国内生产总值50%的阈值下,母体疫苗和单克隆抗体分别在60个和118个国家具有成本效益。
预计这两种干预措施在许多国家都将具有影响力且具有成本效益,如果将针对符合条件国家的特定国家Gavi共同融资纳入其中,这一结果将会得到加强。假设疗效和保护持续时间更高的单克隆抗体,预计在类似价格下比RSV母体疫苗更具成本效益。最终产品特性将影响这一结果。