Department of Cardiothoracic Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.
Department of Cardiothoracic Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.
Ann Thorac Surg. 2023 Jul;116(1):156-162. doi: 10.1016/j.athoracsur.2023.02.062. Epub 2023 Mar 31.
Use of extracorporeal membrane oxygenation (ECMO) as bridge to lung transplant has increased. However, little is known about patients placed on ECMO who die while on the waiting list. Using a national lung transplant data set, we investigated variables associated with waitlist mortality of patients bridged to lung transplant.
All patients supported on ECMO at time of listing were identified using the United Network for Organ Sharing database. Univariable analyses were performed using bias-reduced logistic regression. Cause-specific hazard models were used to determine the effect of variables of interest on hazard of outcomes.
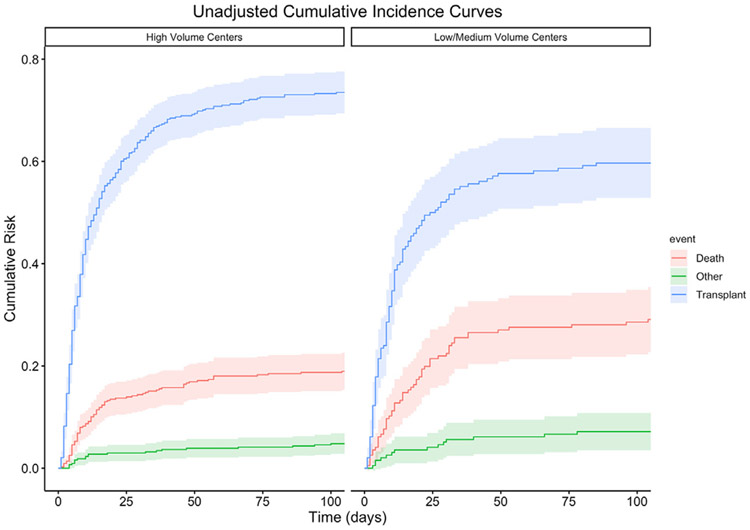
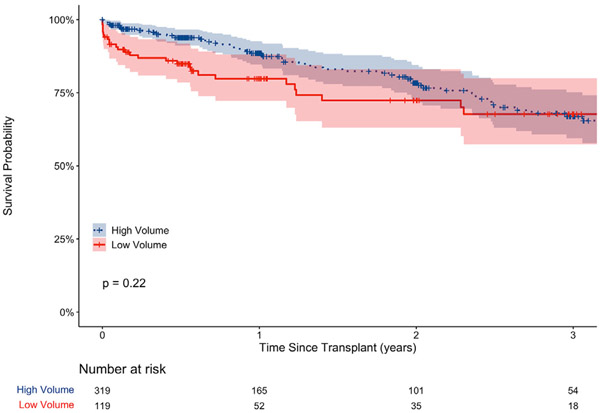
From April 2016 to December 2021, 634 patients met inclusion criteria. Of these, 445 (70%) were successfully bridged to transplant, 148 (23%) died on the waitlist, and 41 (6.5%) were removed for other reasons. Univariable analysis found associations between waitlist mortality and blood group, age, body mass index, serum creatinine, lung allocation score, days on waitlist, United Network for Organ Sharing region, and being listed at a lower-volume center. Cause-specific hazard models demonstrated that patients at high-volume centers were 24% more likely to survive to transplant and 44% less likely to die on the waitlist. Among patients who were successfully bridged to transplant, there was no difference in survival between low- and high-volume centers.
ECMO is an appropriate strategy to bridge selected high-risk patients to lung transplant. Of those placed on ECMO with intent to transplant, about one quarter may not survive to transplantation. High-risk patients requiring advanced support strategies may be more likely to survive to transplant when bridged at a high-volume center.
体外膜肺氧合(ECMO)作为肺移植桥接的应用有所增加。然而,对于在等待名单上死亡的接受 ECMO 治疗的患者,人们知之甚少。本研究利用国家肺移植数据库,调查了与肺移植桥接患者等待名单死亡率相关的变量。
使用美国器官共享网络数据库确定列出名单时接受 ECMO 支持的所有患者。采用偏倚校正逻辑回归进行单变量分析。使用特定于原因的风险模型确定感兴趣变量对结果风险的影响。
2016 年 4 月至 2021 年 12 月,共有 634 名患者符合纳入标准。其中,445 名(70%)成功桥接移植,148 名(23%)在等待名单上死亡,41 名(6.5%)因其他原因被移出。单变量分析发现等待名单死亡率与血型、年龄、体重指数、血清肌酐、肺分配评分、等待时间、美国器官共享网络区域以及在低容量中心列出名单有关。特定于原因的风险模型表明,高容量中心的患者更有可能存活至移植,而在等待名单上死亡的可能性降低 44%。在成功桥接至移植的患者中,低容量和高容量中心之间的生存率没有差异。
ECMO 是将选定的高危患者桥接至肺移植的合适策略。在那些有移植意向并接受 ECMO 治疗的患者中,约有四分之一可能无法存活至移植。需要高级支持策略的高危患者在高容量中心桥接时更有可能存活至移植。