Arafa Mostafa A, Rabah Danny M, Khan Farrukh, Farhat Karim Hamda, Ibrahim Nahla Khamis, Albekairi Alanoud A
The Cancer Research Chair, King Saud University, Riyadh, Saudi Arabia.
Department of Epidemiology, High Institute of Public Health, Alexandria University, Alexandria, Egypt.
Urol Ann. 2023 Jan-Mar;15(1):54-59. doi: 10.4103/ua.ua_22_22. Epub 2022 Nov 8.
False-positive (FP) multiparametric magnetic resonance imaging (MPMRI) obscures and swift needless biopsies in men with a high prostate-specific antigen.
This was a retrospective study, in which all patients who had been exposed to consecutive MP-MRI of the prostate combined with transrectal ultrasound-guided-magnetic resonance imaging fusion-guided prostate biopsy between 2017 and 2020 were involved in the study. The FP was measured as the number of biopsies that did not encompass prostate cancer divided by the whole number of biopsies.
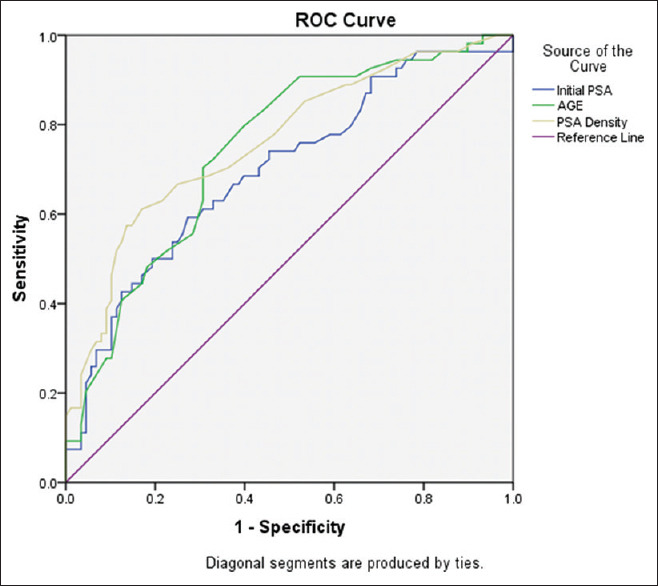
The percentage of FP cases was 51.1%, the highest percentage was found in Prostate Imaging-Reporting and Data System (PI-RADs) 3 (37.7%) and the lowest was detected in PI-RAD 5 (14.5%). Those with FP biopsies are younger, and their total prostate antigen (PSA) and PSA density (PSAD) are significantly lesser. The area under the curve PSAD, age, and total PSA are 0.76, 0.74, and 0.69, respectively. An optimum PSAD value of 0.135 was chosen as a cutoff because it showed the highest sum of sensitivity and specificity, 68% and 69%, respectively.
FP results of mpMRI were detected in more than half of our sample, more than one-third were presented in Pi-RAD3, improved imaging techniques to decrease FP rates are highly needed.
在前列腺特异性抗原水平较高的男性中,多参数磁共振成像(MPMRI)的假阳性(FP)结果会导致不必要的活检并掩盖病情。
这是一项回顾性研究,纳入了2017年至2020年间接受连续前列腺MP-MRI检查并结合经直肠超声引导-磁共振成像融合引导前列腺活检的所有患者。FP的计算方法为未发现前列腺癌的活检次数除以活检总次数。
FP病例的百分比为51.1%,在前列腺影像报告和数据系统(PI-RADs)3中发现的百分比最高(37.7%),在PI-RAD 5中最低(14.5%)。接受FP活检的患者更年轻,其总前列腺抗原(PSA)和PSA密度(PSAD)显著更低。PSAD、年龄和总PSA的曲线下面积分别为0.76、0.74和0.69。选择最佳PSAD值0.135作为临界值,因为它显示出最高的敏感性和特异性之和,分别为68%和69%。
在我们的样本中,超过一半的mpMRI结果为FP,超过三分之一出现在Pi-RAD3中,因此迫切需要改进成像技术以降低FP率。