Henan Joint International Pediatric Urodynamic Laboratory, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, China.
Department of Clinical Laboratory, Key Clinical Laboratory of Henan Province, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, China.
Lipids Health Dis. 2023 Apr 6;22(1):48. doi: 10.1186/s12944-023-01806-2.
Presently, there is no consensus regarding the optimal serum uric acid (SUA) concentration for pediatric patients. Adenoid and tonsillar hypertrophy is considered to be closely associated with pediatric metabolic syndrome and cardiovascular risk and is a common condition in children admitted to the hospital. Therefore, we aimed to evaluate the relationship between SUA and dyslipidemia and propose a reference range for SUA concentration that is associated with a healthy lipid profile in hospitalized children with adenoid and tonsillar hypertrophy.
Preoperative data from 4922 children admitted for elective adenoidectomy and/or tonsillectomy surgery due to adenoid and tonsillar hypertrophy were collected. SUA concentrations were scaled to standard deviation (SD), and SUA deviations were expressed as SD from the mean SUA of children without dyslipidemia.
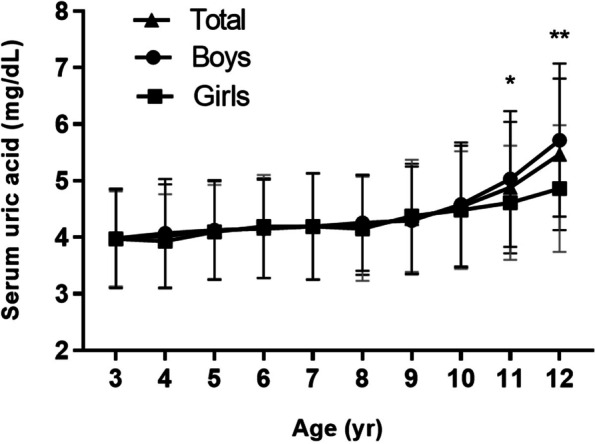
The mean SUA concentration of the participants was 4.27 ± 1.01 mg/dL, and the prevalence of hyperuricemia was 1.6% when it was defined using an SUA of ≥ 7.0 mg/dL. Participants with dyslipidemia (856, 17.4%) had a higher prevalence of hyperuricemia (3.4% vs. 1.2%, P < 0.001) and higher SUA concentrations (4.51 ± 1.15 vs. 4.22 ± 0.97 mg/dL, P < 0.001) than those with ortholiposis. The circulating lipid status of participants with SUAs < 1 SD below the mean value for the participants with ortholiposis (range 1.80-3.28 mg/dL) was more normal. Each 1-SD increase in SUA was associated with a 27% increase in the risk of dyslipidemia (OR = 1.270, 95% CI, 1.185-1.361). Adjustment for a number of potential confounders reduced the strength of the relationship, but this remained significant (OR = 1.125, 95% CI, 1.042-1.215). The higher risk of dyslipidemia was maintained for participants with SUAs > 1 SD above the mean value of the participants with ortholiposis.
SUA was independently associated with dyslipidemia in children with adenoid and tonsillar hypertrophy, and an SUA < 1 SD below the mean value for patients with ortholiposis was associated with a healthy lipid profile.
目前,儿科患者的最佳血清尿酸(SUA)浓度尚无共识。腺样体和扁桃体肥大被认为与儿童代谢综合征和心血管风险密切相关,是腺样体和扁桃体肥大患儿住院的常见病症。因此,我们旨在评估 SUA 与血脂异常的关系,并提出与腺样体和扁桃体肥大患儿健康血脂谱相关的 SUA 浓度参考范围。
收集 4922 例因腺样体和扁桃体肥大行择期腺样体切除术和/或扁桃体切除术的患儿术前数据。将 SUA 浓度标准化为标准差(SD),并将 SUA 偏差表示为无血脂异常儿童平均 SUA 的 SD。
参与者的平均 SUA 浓度为 4.27±1.01mg/dL,当 SUA≥7.0mg/dL 时,高尿酸血症的患病率为 1.6%。患有血脂异常(856 例,17.4%)的患儿高尿酸血症的患病率更高(3.4%比 1.2%,P<0.001),SUA 浓度更高(4.51±1.15 vs. 4.22±0.97mg/dL,P<0.001)。与血脂正常的患儿相比,SUA 值低于血脂正常患儿平均值 1SD 以下的患儿(范围为 1.80-3.28mg/dL),其循环血脂状态更为正常。SUA 每增加 1SD,血脂异常的风险增加 27%(OR=1.270,95%CI,1.185-1.361)。调整多个潜在混杂因素后,该关系的强度有所降低,但仍具有统计学意义(OR=1.125,95%CI,1.042-1.215)。SUA 值高于血脂正常患儿平均值 1SD 以上的患儿,血脂异常的风险仍较高。
SUA 与腺样体和扁桃体肥大患儿的血脂异常独立相关,SUA 值低于血脂正常患儿平均值 1SD 与健康的血脂谱相关。