Department of Cardiovascular Diseases University Hospitals (UZ) Leuven Leuven Belgium.
Department of Radiation Oncology University Hospitals (UZ) Leuven Leuven Belgium.
J Am Heart Assoc. 2023 Apr 18;12(8):e027855. doi: 10.1161/JAHA.122.027855. Epub 2023 Apr 7.
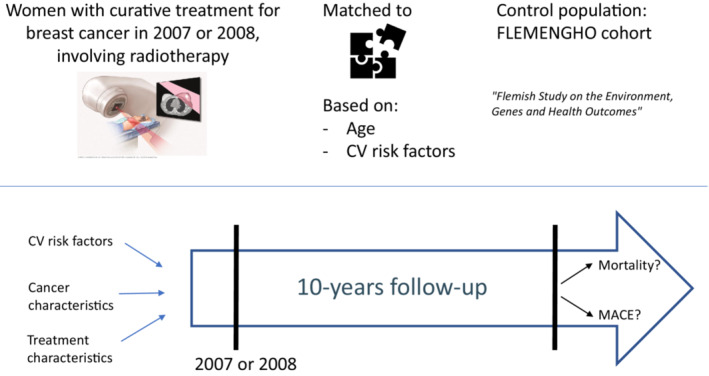
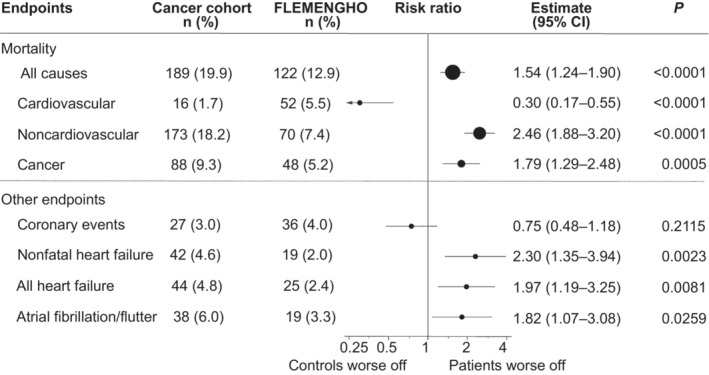
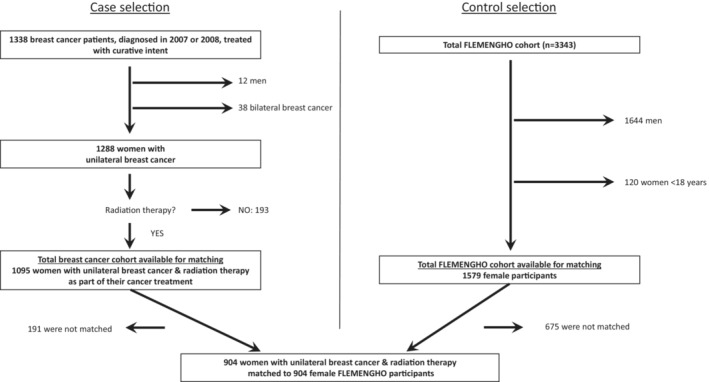
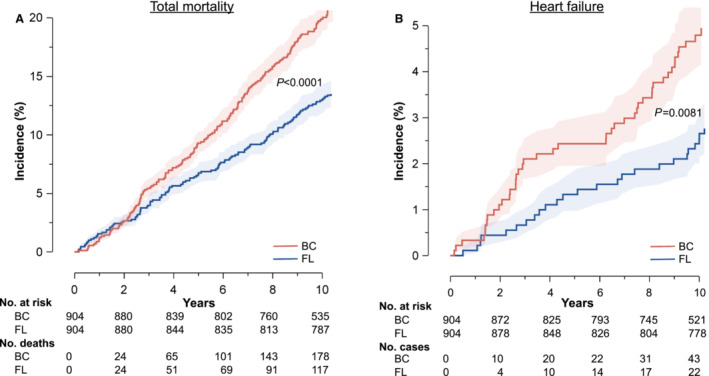
Background Treatment for breast cancer (BC) frequently involves radiotherapy. Guidelines recommend screening for cardiac adverse events starting 10 years after radiotherapy. The rationale for this interval is unclear. Methods and Results We aimed to study cardiovascular event rates in the first decade following curative radiotherapy for BC. We compared mortality and cardiovascular event rates with an age- and risk factor-matched control population. We included 1095 patients with BC (mean age 56±12 years). Two hundred and eighteen (19.9%) women died. Cancer and cardiovascular mortality caused 107 (49.1%) and 22 (10.1%) deaths, respectively. A total of 904 cases were matched to female FLEMENGHO (Flemish Study on Environment, Genes and Health Outcomes) participants. Coronary artery disease incidence was similar (risk ratio [RR], 0.75 [95% CI, 0.48-1.18]), yet heart failure (RR, 1.97 [95% CI, 1.19-3.25]) and atrial fibrillation/flutter (RR, 1.82 [95% CI, 1.07-3.08]) occurred more often in patients with BC. Age (hazard ratio [HR], 1.033 [95% CI, 1.006-1.061], =0.016), tumor grade (HR, 1.739 [95% CI, 1.166-2.591], =0.007), and neoadjuvant treatment setting (HR, 2.782 [95% CI, 1.304-5.936], =0.008) were risk factors for mortality. Risk factors for major adverse cardiac events were age (HR, 1.053 [95% CI, 1.013-1.093]; =0.008), mean heart dose (HR, 1.093 [95% CI, 1.025-1.167]; =0.007), history of cardiovascular disease (HR, 2.386 [95% CI, 1.096-6.197]; =0.029) and Mayo Clinic Cardiotoxicity Risk Score (HR, 2.664 [95% CI, 1.625-4.367]; <0.001). Conclusions Ten-year mortality following curative treatment for unilateral BC was mainly cancer related, but heart failure and atrial fibrillation/flutter were already common in the first decade following irradiation. Mean heart dose, pre-existing cardiovascular diseases, and Mayo Clinic Cardiotoxicity Risk Score were risk factors for cardiac adverse events. These results suggest a need for early dedicated cardio-oncological follow-up after radiotherapy.
乳腺癌(BC)的治疗常包括放疗。指南建议在放疗后 10 年开始筛查心脏不良事件。这种间隔的依据尚不清楚。
我们旨在研究 BC 根治性放疗后第一个十年的心血管事件发生率。我们将死亡率和心血管事件发生率与年龄和危险因素相匹配的对照组进行比较。我们纳入了 1095 例 BC 患者(平均年龄 56±12 岁)。218 名(19.9%)女性死亡。癌症和心血管疾病导致 107 例(49.1%)和 22 例(10.1%)死亡。共有 904 例病例与女性 FLEMENGHO(佛兰德环境、基因和健康结果研究)参与者相匹配。冠心病发病率相似(风险比 [RR],0.75 [95%CI,0.48-1.18]),但心力衰竭(RR,1.97 [95%CI,1.19-3.25])和心房颤动/扑动(RR,1.82 [95%CI,1.07-3.08])在 BC 患者中更为常见。年龄(风险比 [HR],1.033 [95%CI,1.006-1.061],=0.016)、肿瘤分级(HR,1.739 [95%CI,1.166-2.591],=0.007)和新辅助治疗方案(HR,2.782 [95%CI,1.304-5.936],=0.008)是死亡的危险因素。主要不良心脏事件的危险因素是年龄(HR,1.053 [95%CI,1.013-1.093];=0.008)、平均心脏剂量(HR,1.093 [95%CI,1.025-1.167];=0.007)、心血管疾病史(HR,2.386 [95%CI,1.096-6.197];=0.029)和 Mayo 诊所心脏毒性风险评分(HR,2.664 [95%CI,1.625-4.367];<0.001)。
单侧 BC 根治性治疗后 10 年的死亡率主要与癌症有关,但心力衰竭和心房颤动/扑动在放疗后 10 年内已很常见。平均心脏剂量、既往心血管疾病和 Mayo 诊所心脏毒性风险评分是心脏不良事件的危险因素。这些结果表明,放疗后需要早期进行专门的心脏肿瘤学随访。