Kid Risk, Inc., Orlando, FL, United States.
Front Public Health. 2023 Mar 24;11:1098419. doi: 10.3389/fpubh.2023.1098419. eCollection 2023.
Detection of poliovirus transmission and ongoing oral poliovirus vaccine (OPV) use continue to delay poliomyelitis eradication. In 2016, the Global Polio Eradication Initiative (GPEI) coordinated global cessation of type 2 OPV (OPV2) for preventive immunization and limited its use to emergency outbreak response. In 2019, GPEI partners requested restart of some Sabin OPV2 production and also accelerated the development of a genetically modified novel OPV2 vaccine (nOPV2) that promised greater genetic stability than monovalent Sabin OPV2 (mOPV2).
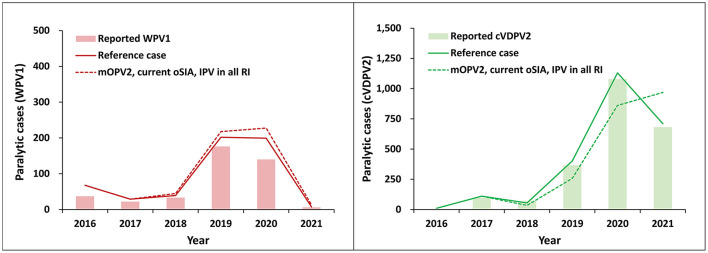
We reviewed integrated risk, economic, and global poliovirus transmission modeling performed before OPV2 cessation, which recommended multiple risk management strategies to increase the chances of successfully ending all transmission of type 2 live polioviruses. Following OPV2 cessation, strategies implemented by countries and the GPEI deviated from model recommended risk management strategies. Complementing other modeling that explores prospective outbreak response options for improving outcomes for the current polio endgame trajectory, in this study we roll back the clock to 2017 and explore counterfactual trajectories that the polio endgame could have followed if GPEI had: (1) managed risks differently after OPV2 cessation and/or (2) developed nOPV2 before and used it exclusively for outbreak response after OPV2 cessation.
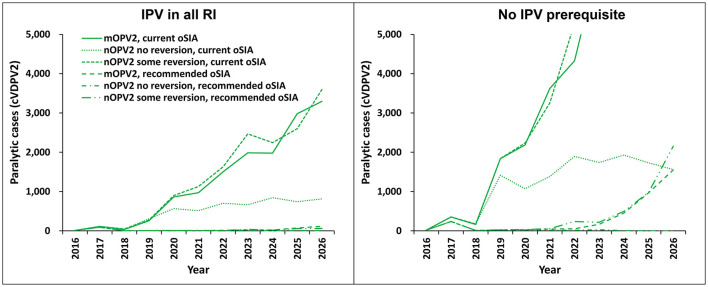
The implementation of the 2016 model-based recommended outbreak response strategies could have ended (and could still substantially improve the probability of ending) type 2 poliovirus transmission. Outbreak response performance observed since 2016 would not have been expected to achieve OPV2 cessation with high confidence, even with the availability of nOPV2 prior to the 2016 OPV2 cessation.
As implemented, the 2016 OPV2 cessation failed to stop type 2 transmission. While nOPV2 offers benefits of lower risk of seeding additional outbreaks, its reduced secondary spread relative to mOPV2 may imply relatively higher coverage needed for nOPV2 than mOPV2 to stop outbreaks.
病毒传播的检测和正在进行的口服脊髓灰质炎疫苗(OPV)的使用继续延迟脊髓灰质炎的根除。2016 年,全球脊髓灰质炎根除倡议(GPEI)协调全球停止使用 2 型口服脊髓灰质炎疫苗(OPV2)进行预防免疫,并将其使用限制在紧急疫情应对。2019 年,GPEI 合作伙伴要求重启一些萨宾 OPV2 生产,并加速开发一种遗传修饰的新型 OPV2 疫苗(nOPV2),该疫苗有望比单价萨宾 OPV2(mOPV2)具有更高的遗传稳定性。
我们回顾了在 OPV2 停止使用之前进行的综合风险、经济和全球脊髓灰质炎病毒传播建模,该建模建议了多种风险管理策略,以增加成功根除所有 2 型活脊髓灰质炎病毒传播的机会。OPV2 停止使用后,各国和 GPEI 实施的策略偏离了模型推荐的风险管理策略。除了其他探索改善当前脊髓灰质炎终结轨迹爆发应对选择的前瞻性建模外,在本研究中,我们回溯到 2017 年,并探索了 GPEI 可能采取的以下两种反事实轨迹:(1)OPV2 停止使用后管理风险的方式不同,和/或(2)在 OPV2 停止使用之前开发 nOPV2 并将其专门用于 OPV2 停止后的疫情应对。
实施 2016 年基于模型推荐的爆发应对策略本可以结束(并且仍然可以大大提高结束的概率)2 型脊髓灰质炎病毒传播。自 2016 年以来观察到的疫情应对表现预计不会有很高的信心实现 OPV2 停止,即使在 2016 年 OPV2 停止之前就有 nOPV2 可用。
正如实施的那样,2016 年 OPV2 停止未能阻止 2 型传播。虽然 nOPV2 具有引发额外疫情风险较低的优势,但与 mOPV2 相比,其继发性传播减少可能意味着 nOPV2 比 mOPV2 停止疫情需要更高的覆盖率。