MRC Unit The Gambia at the London School of Hygiene and Tropical Medicine, Banjul, The Gambia.
Research and Development Division, PT Bio Farma, Bandung, Indonesia.
Lancet. 2024 Mar 23;403(10432):1164-1175. doi: 10.1016/S0140-6736(23)02844-1. Epub 2024 Feb 22.
Novel oral poliovirus vaccine type 2 (nOPV2) has been engineered to improve the genetic stability of Sabin oral poliovirus vaccine (OPV) and reduce the emergence of circulating vaccine-derived polioviruses. This trial aimed to provide key safety and immunogenicity data required for nOPV2 licensure and WHO prequalification.
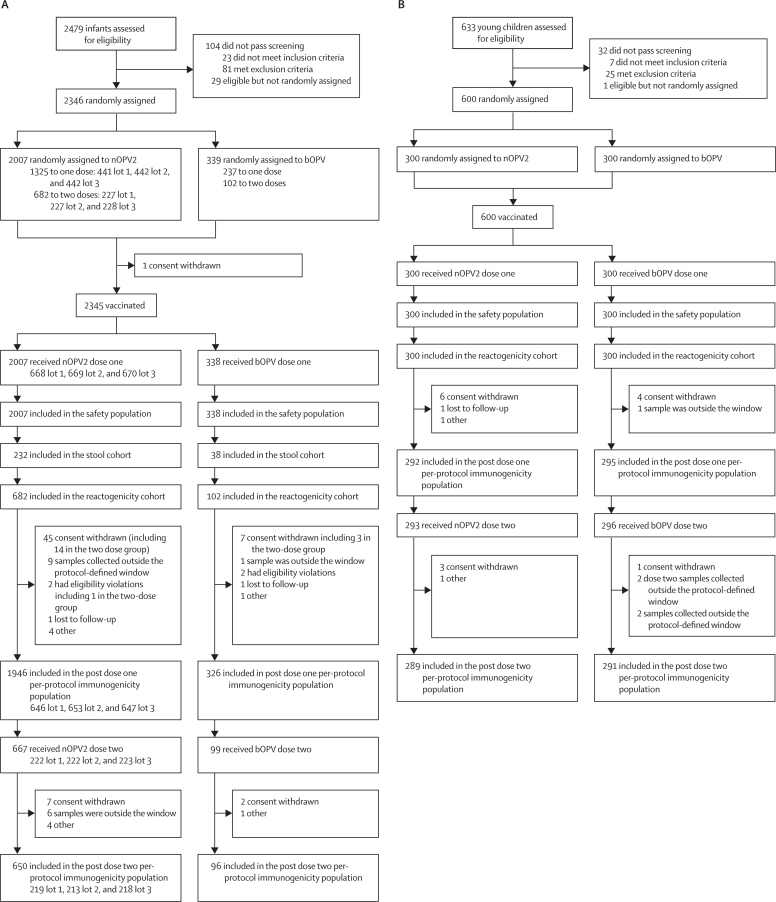
This phase 3 trial recruited infants aged 18 to <52 weeks and young children aged 1 to <5 years in The Gambia. Infants randomly assigned to receive one or two doses of one of three lots of nOPV2 or one lot of bivalent OPV (bOPV). Young children were randomised to receive two doses of nOPV2 lot 1 or bOPV. The primary immunogenicity objective was to assess lot-to-lot equivalence of the three nOPV2 lots based on one-dose type 2 poliovirus neutralising antibody seroconversion rates in infants. Equivalence was declared if the 95% CI for the three pairwise rate differences was within the -10% to 10% equivalence margin. Tolerability and safety were assessed based on the rates of solicited adverse events to 7 days, unsolicited adverse events to 28 days, and serious adverse events to 3 months post-dose. Stool poliovirus excretion was examined. The trial was registered as PACTR202010705577776 and is completed.
Between February and October, 2021, 2345 infants and 600 young children were vaccinated. 2272 (96·9%) were eligible for inclusion in the post-dose one per-protocol population. Seroconversion rates ranged from 48·9% to 49·2% across the three lots. The minimum lower bound of the 95% CIs for the pairwise differences in seroconversion rates between lots was -5·8%. The maximum upper bound was 5·4%. Equivalence was therefore shown. Of those seronegative at baseline, 143 (85·6%) of 167 (95% CI 79·4-90·6) infants and 54 (83·1%) of 65 (71·7-91·2) young children seroconverted over the two-dose nOPV2 schedule. The post-two-dose seroprotection rates, including participants who were both seronegative and seropositive at baseline, were 604 (92·9%) of 650 (95% CI 90·7-94·8) in infants and 276 (95·5%) of 289 (92·4-97·6) in young children. No safety concerns were identified. 7 days post-dose one, 78 (41·7%) of 187 (95% CI 34·6-49·1) infants were excreting the type 2 poliovirus.
nOPV2 was immunogenic and safe in infants and young children in The Gambia. The data support the licensure and WHO prequalification of nOPV2.
Bill & Melinda Gates Foundation.
新型口服脊髓灰质炎病毒 2 型(nOPV2)经过工程改造,提高了萨宾口服脊髓灰质炎疫苗(OPV)的遗传稳定性,并降低了循环疫苗衍生脊髓灰质炎病毒的出现。这项试验旨在提供 nOPV2 许可和世卫组织预认证所需的关键安全性和免疫原性数据。
这项 3 期试验在冈比亚招募了 18 至<52 周龄的婴儿和 1 至<5 岁的幼儿。婴儿随机分配接受三种剂量的 nOPV2 中的一种或两种,或一种双价 OPV(bOPV)。幼儿随机接受 nOPV2 1 号剂量的两剂或 bOPV。主要免疫原性目标是根据婴儿中一剂 2 型脊髓灰质炎病毒中和抗体血清转化率评估三种 nOPV2 剂量的批间等效性。如果三个两两差异率的 95%置信区间在-10%至 10%的等效性区间内,则宣布等效性。基于 7 天内的不良事件发生率、28 天内的不良事件发生率和 3 个月内的不良事件发生率,评估了耐受性和安全性。检测粪便中的脊髓灰质炎病毒排泄情况。该试验在 PACTR202010705577776 注册,并已完成。
2021 年 2 月至 10 月,2345 名婴儿和 600 名幼儿接受了疫苗接种。2272 名(96.9%)符合入组条件。血清转化率在三种剂量之间的范围为 48.9%至 49.2%。批间差异血清转化率最低下限 95%置信区间为-5.8%。上限最高为 5.4%。因此证明了等效性。在基线时血清阴性的 167 名婴儿(95%置信区间 79.4-90.6)中,143 名(85.6%)和 65 名幼儿(91.7-91.2)中 54 名(83.1%)在接受两剂 nOPV2 方案后血清转化。包括基线时血清阴性和阳性的参与者,2 剂 nOPV2 后的血清保护率为 650 名(95%置信区间 90.7-94.8)中的 604 名(92.9%)婴儿和 289 名(92.4-97.6)中的 276 名(95.5%)幼儿。未发现安全性问题。在接种后 1 天,187 名婴儿(95%置信区间 34.6-49.1)中有 78 名(41.7%)排泄 2 型脊髓灰质炎病毒。
nOPV2 在冈比亚的婴儿和幼儿中具有免疫原性和安全性。这些数据支持 nOPV2 的许可和世卫组织预认证。
比尔及梅琳达·盖茨基金会。