Rejeski Kai, Blumenberg Viktoria, Iacoboni Gloria, Lopez-Corral Lucia, Kharboutli Soraya, Hernani Rafael, Petrera Agnese, Müller Niklas, Hildebrand Friederike, Frölich Lisa, Karschnia Philipp, Schmidt Christian, Cordas Dos Santos David M, Piñana José Luis, Müller Fabian, Martin Ana Africa, Dreyling Martin, von Bergwelt-Baildon Michael, Barba Pere, Subklewe Marion, Bücklein Veit L
Department of Medicine III - Hematology/Oncology, University Hospital, LMU Munich, Germany.
Laboratory for Translational Cancer Immunology, LMU Gene Center, Munich, Germany.
Hemasphere. 2023 Apr 5;7(4):e858. doi: 10.1097/HS9.0000000000000858. eCollection 2023 Apr.
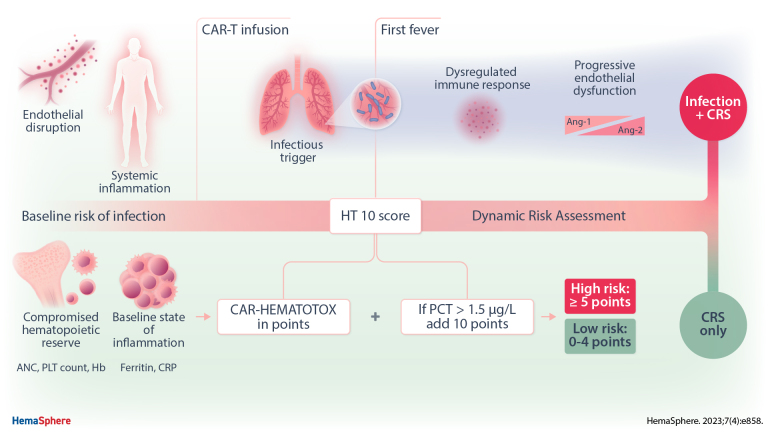
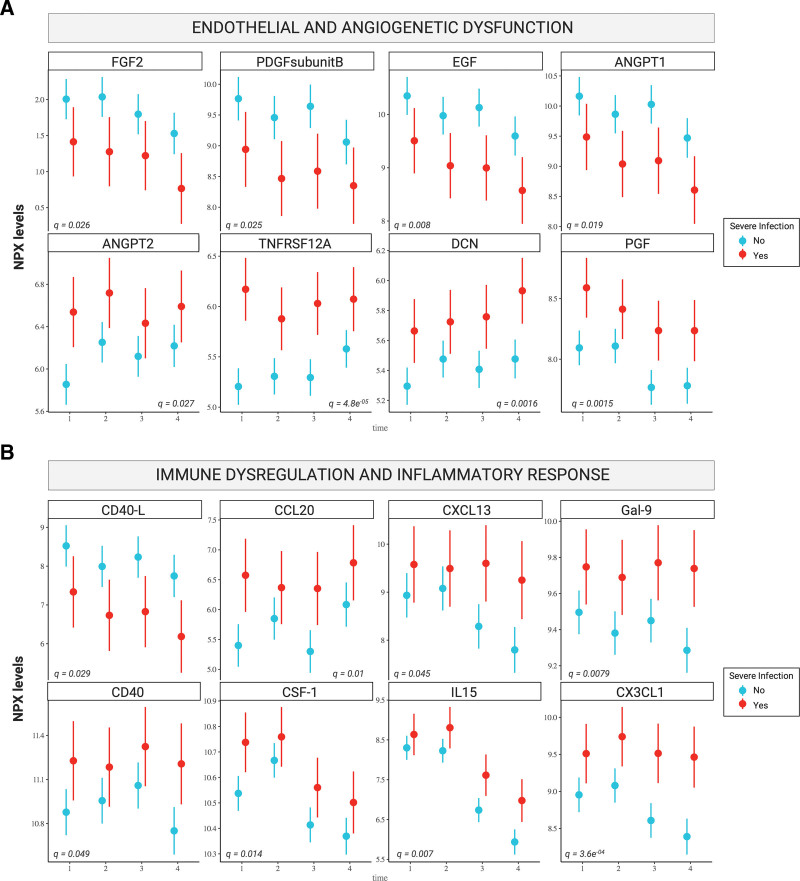
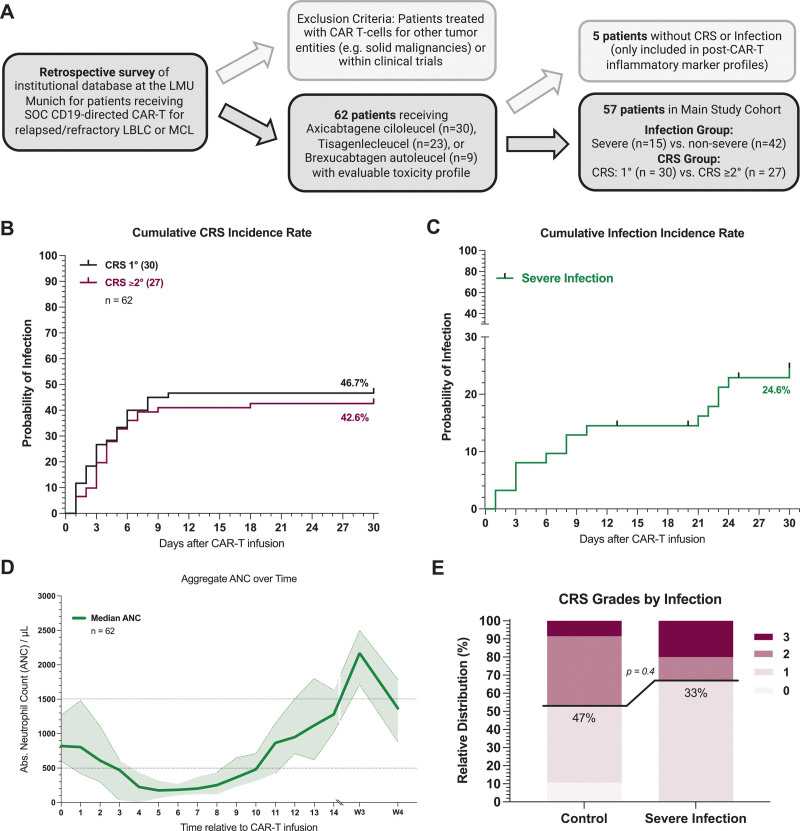
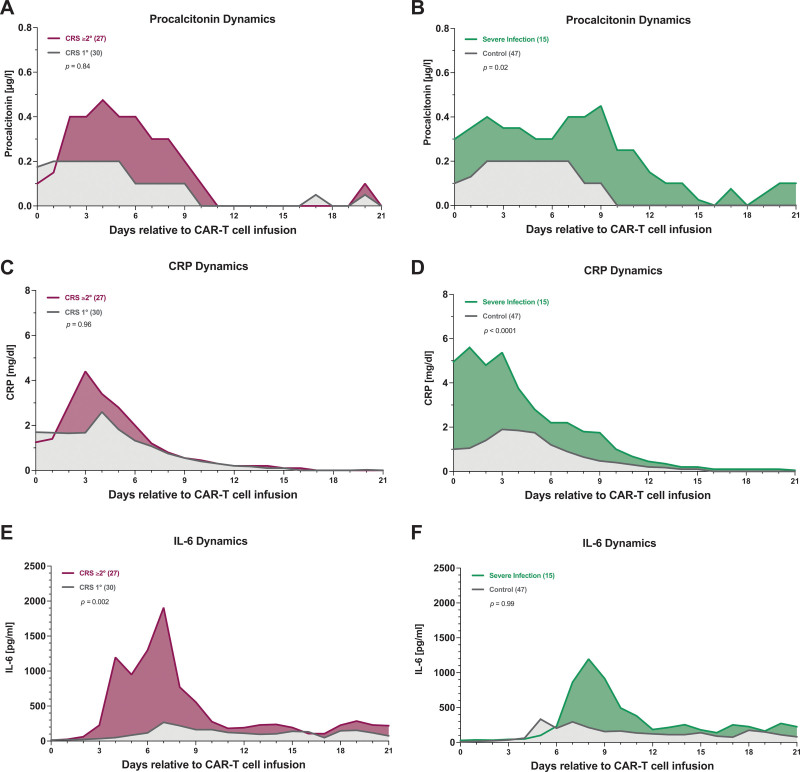
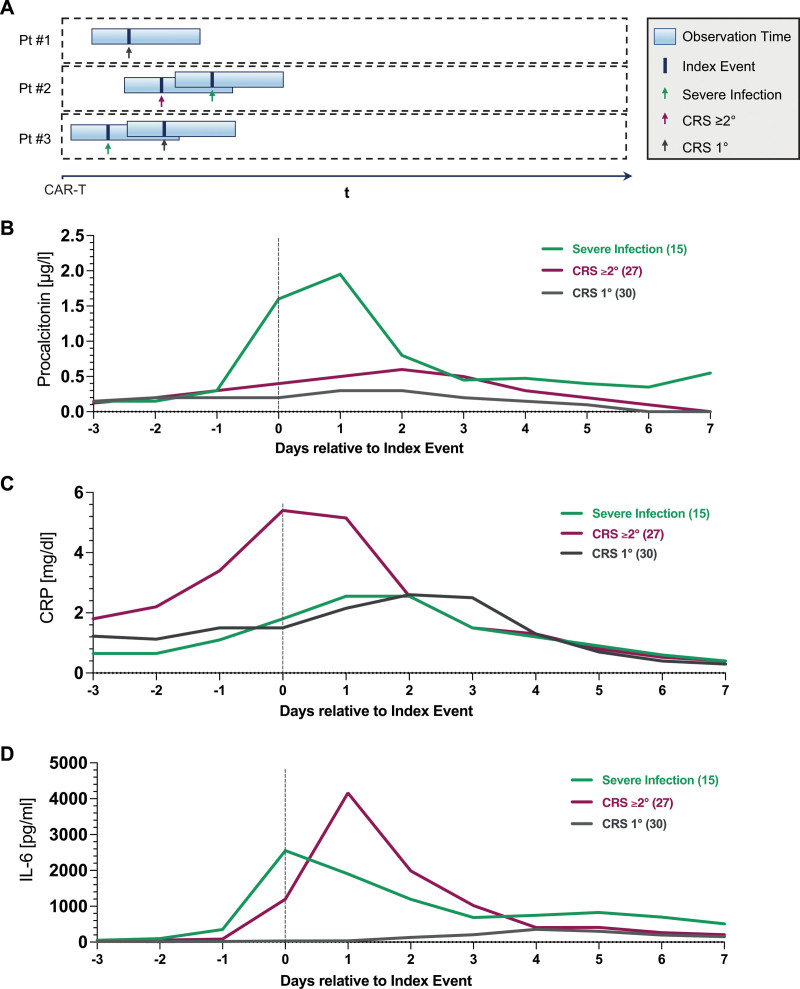
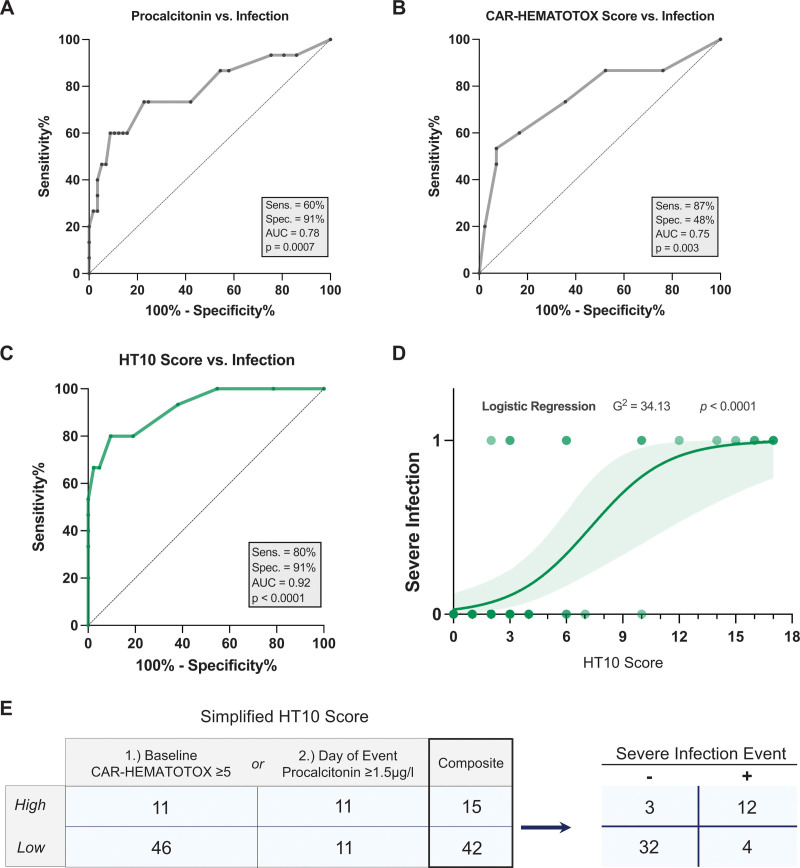
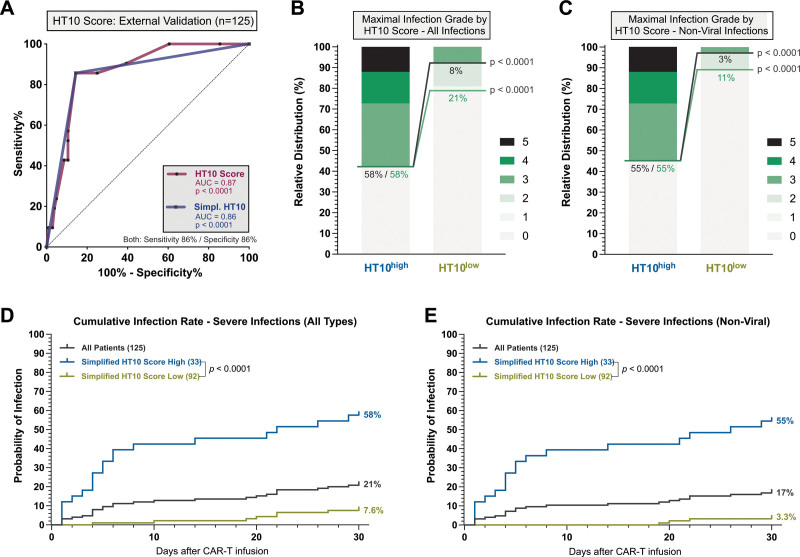
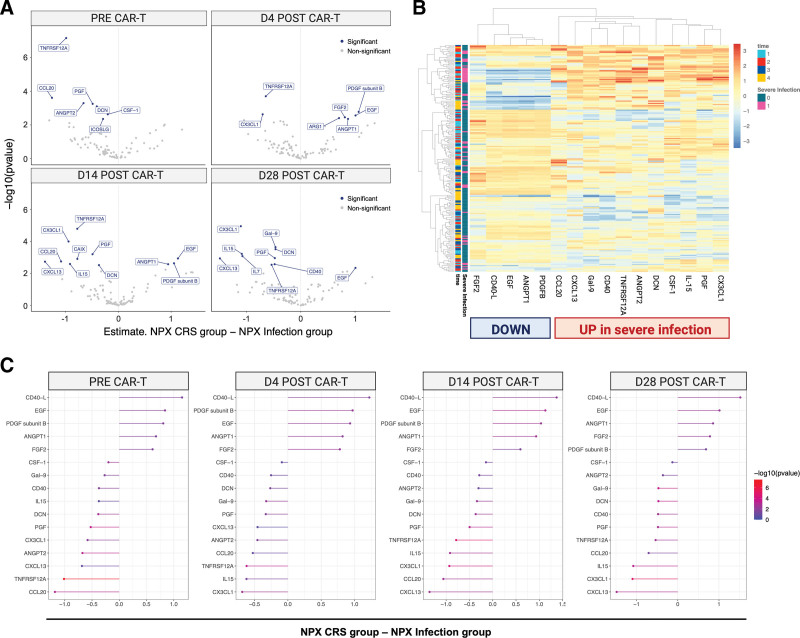
Early fever after chimeric antigen receptor T-cell (CAR-T) therapy can reflect both an infection or cytokine release syndrome (CRS). Identifying early infections in the setting of CRS and neutropenia represents an unresolved clinical challenge. In this retrospective observational analysis, early fever events (day 0-30) were characterized as infection versus CRS in 62 patients treated with standard-of-care CD19.CAR-T for relapsed/refractory B-cell non-Hodgkin lymphoma. Routine serum inflammatory markers (C-reactive protein [CRP], interleukin-6 [IL-6], procalcitonin [PCT]) were recorded daily. Exploratory plasma proteomics were performed longitudinally in 52 patients using a multiplex proximity extension assay (Olink proteomics). Compared with the CRS cohort, we noted increased event-day IL-6 (median 2243 versus 64 pg/mL, = 0.03) and particularly high PCT levels (median 1.6 versus 0.3 µg/L, < 0.0001) in the patients that developed severe infections. For PCT, an optimal discriminatory threshold of 1.5 µg/L was established (area under the receiver operating characteristic curve [AUC] = 0.78). Next, we incorporated day-of-fever PCT levels with the patient-individual CAR-HEMATOTOX score. In a multicenter validation cohort (n = 125), we confirmed the discriminatory capacity of this so-called HT10 score for early infections at first fever (AUC = 0.87, < 0.0001, sens. 86%, spec. 86%). Additionally, Olink proteomics revealed pronounced immune dysregulation and endothelial dysfunction in patients with severe infections as evidenced by an increased ANGPT2/1 ratio and an altered CD40/CD40L-axis. In conclusion, the high discriminatory capacity of the HT10 score for infections highlights the advantage of dynamic risk assessment and supports the incorporation of PCT into routine inflammatory panels. Candidate markers from Olink proteomics may further refine risk-stratification. If validated prospectively, the score will enable risk-adapted decisions on antibiotic use.
嵌合抗原受体T细胞(CAR-T)疗法后的早期发热可能反映感染或细胞因子释放综合征(CRS)。在CRS和中性粒细胞减少的情况下识别早期感染是一个尚未解决的临床挑战。在这项回顾性观察分析中,对62例接受标准治疗的CD19.CAR-T治疗复发/难治性B细胞非霍奇金淋巴瘤的患者,将早期发热事件(第0 - 30天)分为感染与CRS。每天记录常规血清炎症标志物(C反应蛋白[CRP]、白细胞介素-6[IL-6]、降钙素原[PCT])。使用多重邻位延伸分析(Olink蛋白质组学)对52例患者进行纵向探索性血浆蛋白质组学研究。与CRS队列相比,我们注意到发生严重感染的患者在事件日IL-6升高(中位数2243对64 pg/mL,P = 0.03),特别是PCT水平非常高(中位数1.6对0.3 μg/L,P < 0.0001)。对于PCT,确定了1.5 μg/L的最佳鉴别阈值(受试者操作特征曲线下面积[AUC] = 0.78)。接下来,我们将发热日PCT水平与患者个体的CAR-HEMATOTOX评分相结合。在一个多中心验证队列(n = 125)中,我们证实了这个所谓的HT10评分在首次发热时对早期感染的鉴别能力(AUC = 0.87,P < 0.0001,敏感性86%,特异性86%)。此外,Olink蛋白质组学显示严重感染患者存在明显的免疫失调和内皮功能障碍,表现为ANGPT2/1比值升高和CD40/CD40L轴改变。总之,HT10评分对感染的高鉴别能力突出了动态风险评估的优势,并支持将PCT纳入常规炎症指标检测。Olink蛋白质组学的候选标志物可能进一步优化风险分层。如果前瞻性验证成功,该评分将有助于对抗生素使用做出风险适应性决策。