Research Group Cardiovascular Diseases, GENCOR Department, University of Antwerp, Antwerp, Belgium.
Department of Cardiology, Antwerp University Hospital (UZA), Edegem, Belgium.
ESC Heart Fail. 2021 Aug;8(4):2741-2754. doi: 10.1002/ehf2.13344. Epub 2021 May 2.
Heart failure (HF) guidelines place patients into 3 discrete groups according to left ventricular ejection fraction (LVEF): reduced (<40%), mid-range (40-49%), and preserved LVEF (≥50%). We assessed whether clinical phenogroups offer better prognostication than LVEF.
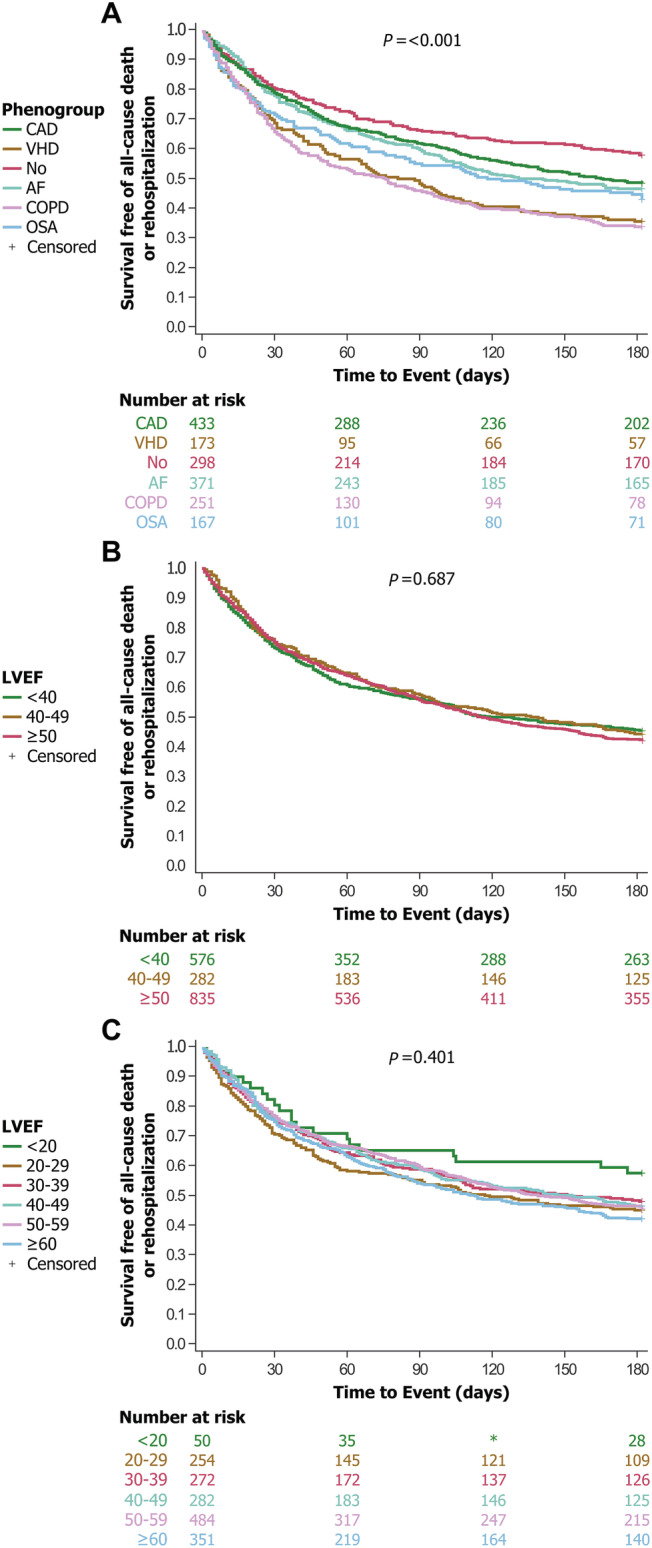
This was a sub-study of the Patient-Centered Care Transitions in HF trial. We analysed baseline characteristics of hospitalized patients in whom LVEF was recorded. We used unsupervised machine learning to identify clinical phenogroups and, thereafter, determined associations between phenogroups and outcomes. Primary outcome was the composite of all-cause death or rehospitalization at 6 and 12 months. Secondary outcome was the composite cardiovascular death or HF rehospitalization at 6 and 12 months. Cluster analysis of 1693 patients revealed six discrete phenogroups, each characterized by a predominant comorbidity: coronary heart disease, valvular heart disease, atrial fibrillation (AF), sleep apnoea, chronic obstructive pulmonary disease (COPD), or few comorbidities. Phenogroups were LVEF independent, with each phenogroup encompassing a wide range of LVEFs. For the primary composite outcome at 6 months, the hazard ratios (HRs) for phenogroups ranged from 1.25 [95% confidence interval (CI) 1.00-1.58 for AF] to 2.04 (95% CI 1.62-2.57 for COPD) (log-rank P < 0.001); and at 12 months, the HRs for phenogroups ranged from 1.15 (95% CI 0.94-1.41 for AF) to 1.87 (95% 1.52-3.20 for COPD) (P < 0.002). LVEF-based classifications did not separate patients into different risk categories for the primary outcomes at 6 months (P = 0.69) and 12 months (P = 0.30). Phenogroups also stratified risk of the secondary composite outcome at 6 and 12 months more effectively than LVEF.
Among patients hospitalized for HF, clinical phenotypes generated by unsupervised machine learning provided greater prognostic information for a composite of clinical endpoints at 6 and 12 months compared with LVEF-based categories.
ClinicalTrials.gov Identifier: NCT02112227.
心力衰竭(HF)指南根据左心室射血分数(LVEF)将患者分为 3 个离散组:射血分数降低(<40%)、中间范围(40-49%)和射血分数保留(≥50%)。我们评估了临床表型是否比 LVEF 提供更好的预后。
这是心力衰竭患者以患者为中心的护理过渡试验的子研究。我们分析了记录 LVEF 的住院患者的基线特征。我们使用无监督机器学习来识别临床表型,然后确定表型与结局之间的关联。主要结局是 6 个月和 12 个月时全因死亡或再住院的复合结局。次要结局是 6 个月和 12 个月时心血管死亡或 HF 再住院的复合结局。对 1693 名患者进行聚类分析,揭示了六个离散的表型组,每个组都有一个主要的合并症:冠心病、瓣膜性心脏病、心房颤动(AF)、睡眠呼吸暂停、慢性阻塞性肺疾病(COPD)或合并症较少。表型与 LVEF 无关,每个表型组都包含广泛的 LVEF 范围。对于 6 个月时的主要复合结局,表型的风险比(HRs)范围为 1.25(95%置信区间[CI]为 1.00-1.58)至 2.04(95%CI 为 1.62-2.57)(对数秩 P<0.001);在 12 个月时,表型的 HR 范围为 1.15(95%CI 为 0.94-1.41)至 1.87(95%CI 为 1.52-3.20)(P<0.002)。基于 LVEF 的分类在 6 个月(P=0.69)和 12 个月(P=0.30)时无法将患者分为不同的风险类别。表型还比 LVEF 更有效地分层 6 个月和 12 个月时次要复合结局的风险。
在因 HF 住院的患者中,无监督机器学习生成的临床表型在 6 个月和 12 个月时的复合临床终点的预后信息优于基于 LVEF 的分类。
ClinicalTrials.gov 标识符:NCT02112227。