Gelderblom Mathias, Koch Simon, Strecker Jan-Kolja, Jørgensen Carina, Garcia-Bonilla Lidia, Ludewig Peter, Schädlich Ines Sophie, Piepke Marius, Degenhardt Karoline, Bernreuther Christian, Pinnschmidt Hans, Arumugam Thiruma V, Thomalla Götz, Faber Cornelius, Sedlacik Jan, Gerloff Christian, Minnerup Jens, Clausen Bettina H, Anrather Josef, Magnus Tim
Department of Neurology, University Medical Center Hamburg-Eppendorf, 20246 Hamburg, Germany.
Department of Neurology with Institute of Translational Neurology, University of Münster, 48149 Münster, Germany.
Brain Commun. 2023 Mar 23;5(2):fcad090. doi: 10.1093/braincomms/fcad090. eCollection 2023.
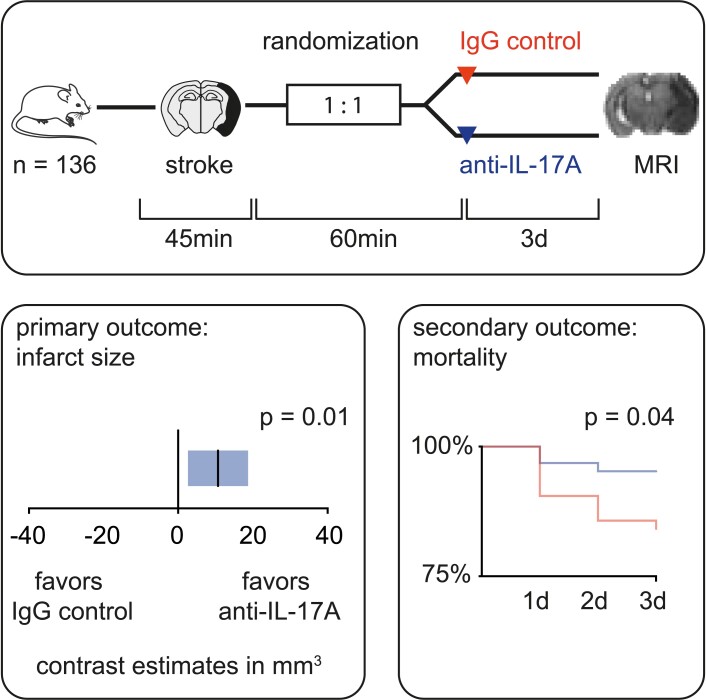
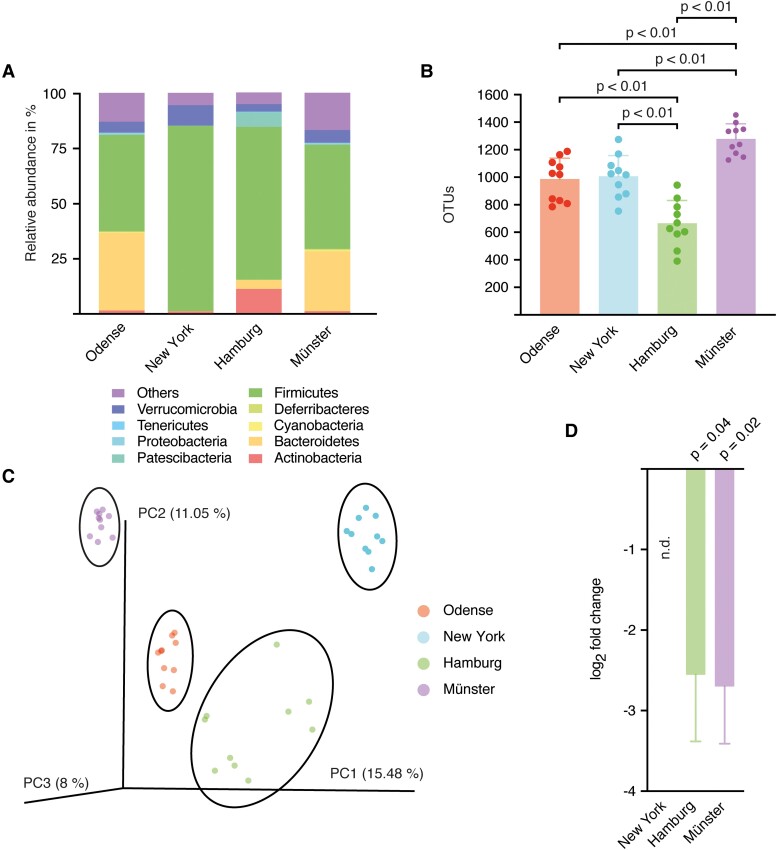
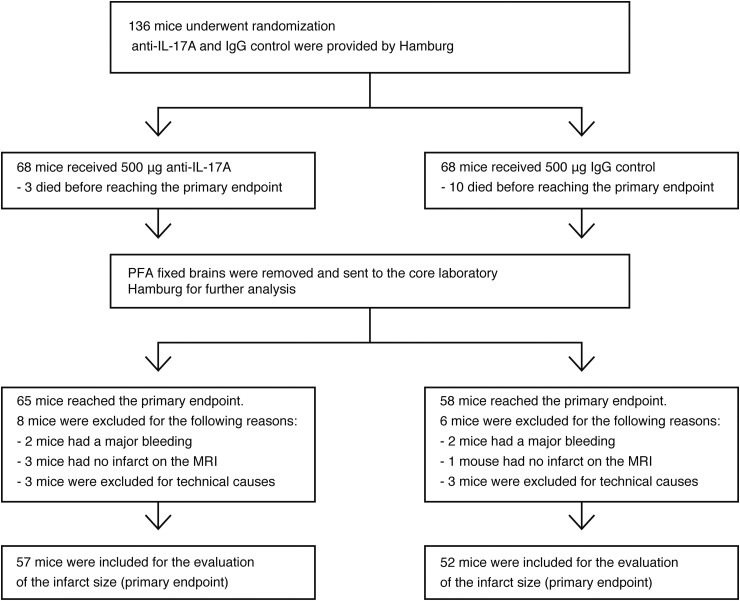
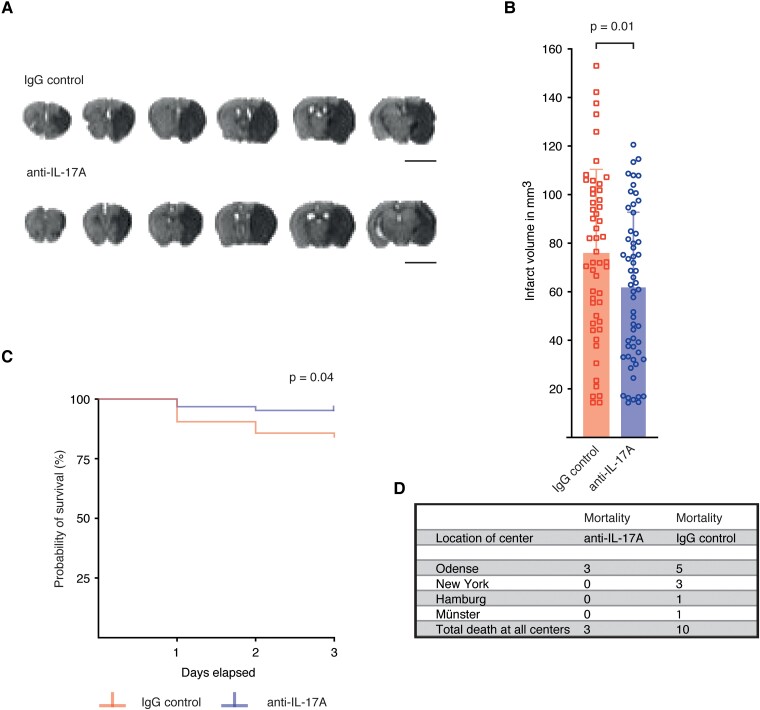
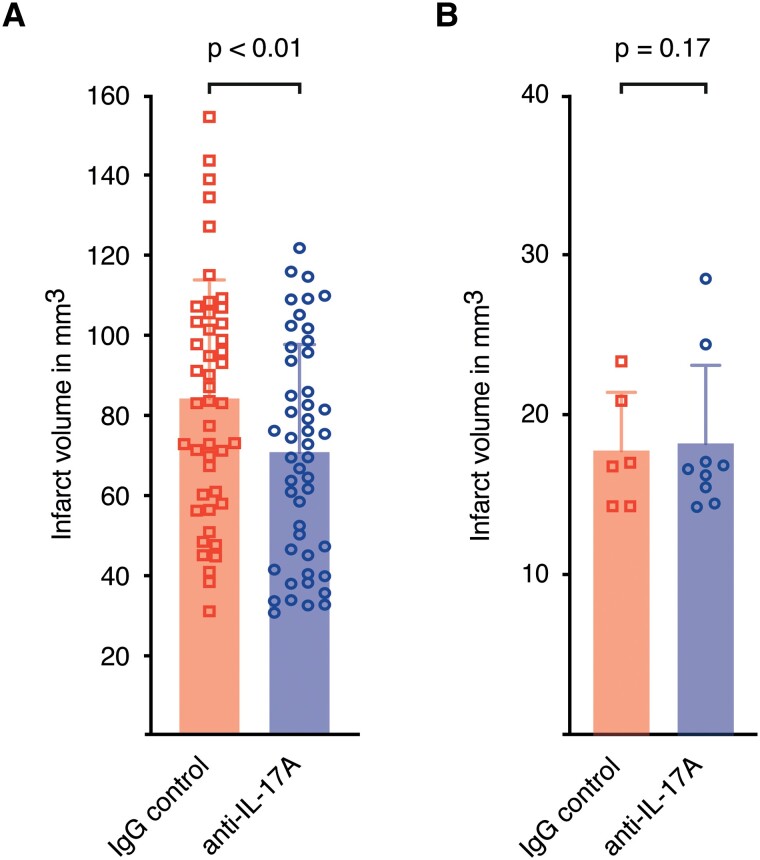
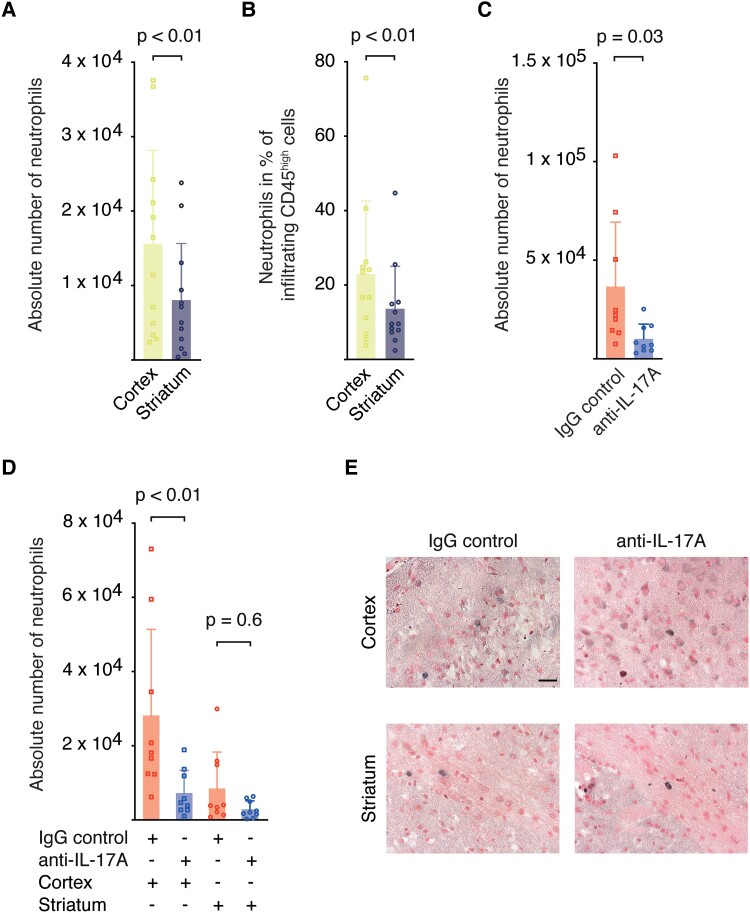
Multiple consensus statements have called for preclinical randomized controlled trials to improve translation in stroke research. We investigated the efficacy of an interleukin-17A neutralizing antibody in a multi-centre preclinical randomized controlled trial using a murine ischaemia reperfusion stroke model. Twelve-week-old male C57BL/6 mice were subjected to 45 min of transient middle cerebral artery occlusion in four centres. Mice were randomly assigned (1:1) to receive either an anti-interleukin-17A (500 µg) or isotype antibody (500 µg) intravenously 1 h after reperfusion. The primary endpoint was infarct volume measured by magnetic resonance imaging three days after transient middle cerebral artery occlusion. Secondary analysis included mortality, neurological score, neutrophil infiltration and the impact of the gut microbiome on treatment effects. Out of 136 mice, 109 mice were included in the analysis of the primary endpoint. Mixed model analysis revealed that interleukin-17A neutralization significantly reduced infarct sizes (anti-interleukin-17A: 61.77 ± 31.04 mm; IgG control: 75.66 ± 34.79 mm; = 0.01). Secondary outcome measures showed a decrease in mortality (hazard ratio = 3.43, 95% confidence interval = 1.157-10.18; = 0.04) and neutrophil invasion into ischaemic cortices (anti-interleukin-17A: 7222 ± 6108 cells; IgG control: 28 153 ± 23 206 cells; < 0.01). There was no difference in Bederson score. The analysis of the gut microbiome showed significant heterogeneity between centres ( = 0.78, < 0.001, = 40). Taken together, neutralization of interleukin-17A in a therapeutic time window resulted in a significant reduction of infarct sizes and mortality compared with isotype control. It suggests interleukin-17A neutralization as a potential therapeutic target in stroke.
多项共识声明呼吁开展临床前随机对照试验,以改善中风研究中的转化。我们在一项多中心临床前随机对照试验中,使用小鼠缺血再灌注中风模型,研究了白细胞介素-17A中和抗体的疗效。12周龄雄性C57BL/6小鼠在四个中心接受45分钟的短暂大脑中动脉闭塞。小鼠在再灌注1小时后随机分配(1:1)静脉注射抗白细胞介素-17A(500μg)或同型抗体(500μg)。主要终点是短暂大脑中动脉闭塞三天后通过磁共振成像测量的梗死体积。次要分析包括死亡率、神经学评分、中性粒细胞浸润以及肠道微生物群对治疗效果的影响。在136只小鼠中,109只小鼠被纳入主要终点分析。混合模型分析显示,白细胞介素-17A中和显著减小了梗死面积(抗白细胞介素-17A:61.77±31.04mm;IgG对照:75.66±34.79mm;P = 0.01)。次要结局指标显示死亡率降低(风险比=3.43,95%置信区间=1.157 - 10.18;P = 0.04),并且中性粒细胞向缺血皮质的浸润减少(抗白细胞介素-17A:7222±6108个细胞;IgG对照:28153±23206个细胞;P < 0.01)。贝德森评分无差异。肠道微生物群分析显示各中心之间存在显著异质性(I² = 0.78,P < 0.001,df = 40)。总体而言,与同型对照相比,在治疗时间窗内中和白细胞介素-17A可显著减小梗死面积并降低死亡率。这表明白细胞介素-17A中和作为中风的潜在治疗靶点。