Department of Diagnostic and Interventional Radiology, University Medical Center Freiburg, Faculty of Medicine, University of Freiburg, Germany.
Berta-Ottenstein-Programme, University of Freiburg, Faculty of Medicine, Freiburg, Germany.
Theranostics. 2023 Mar 5;13(5):1594-1606. doi: 10.7150/thno.81938. eCollection 2023.
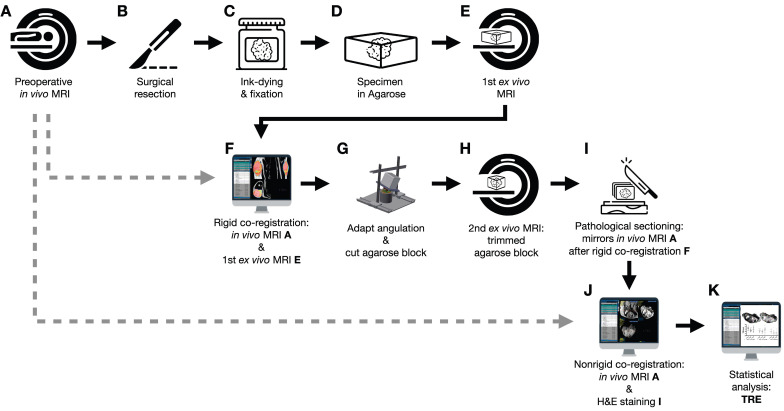
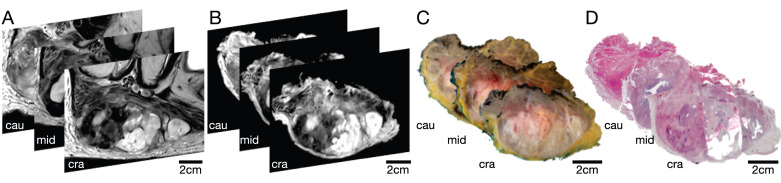
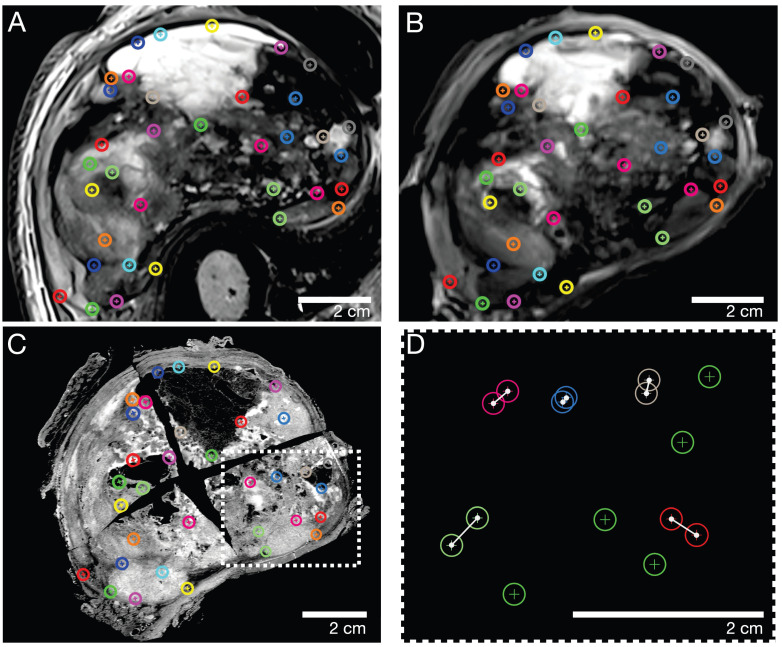
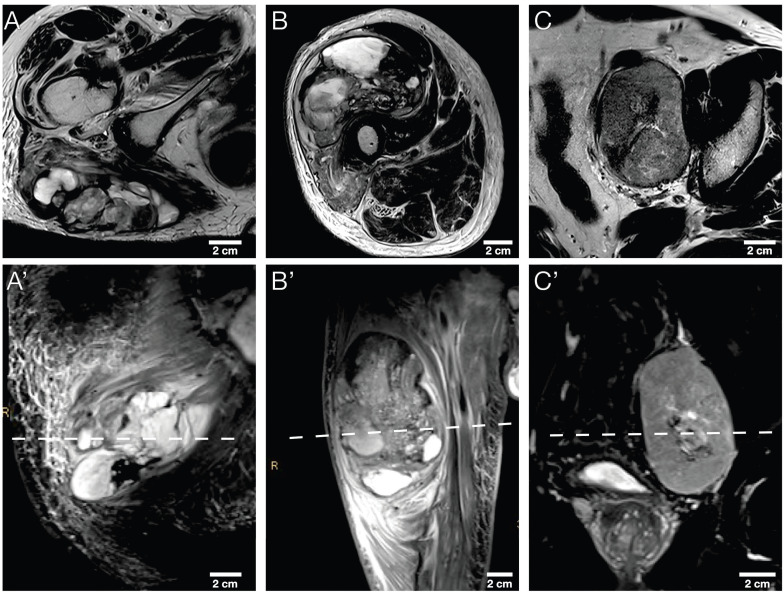
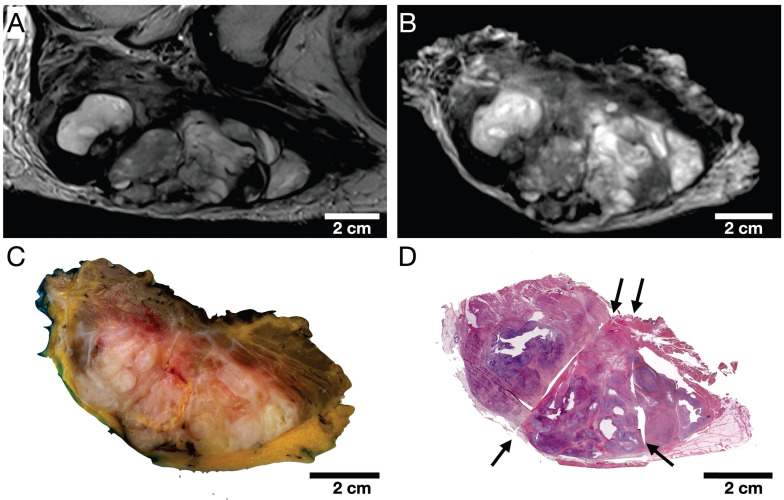
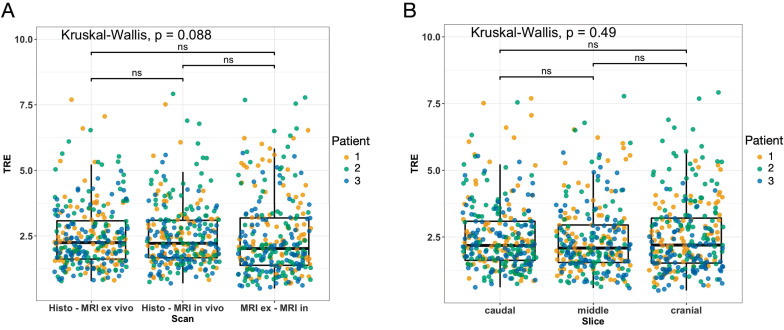
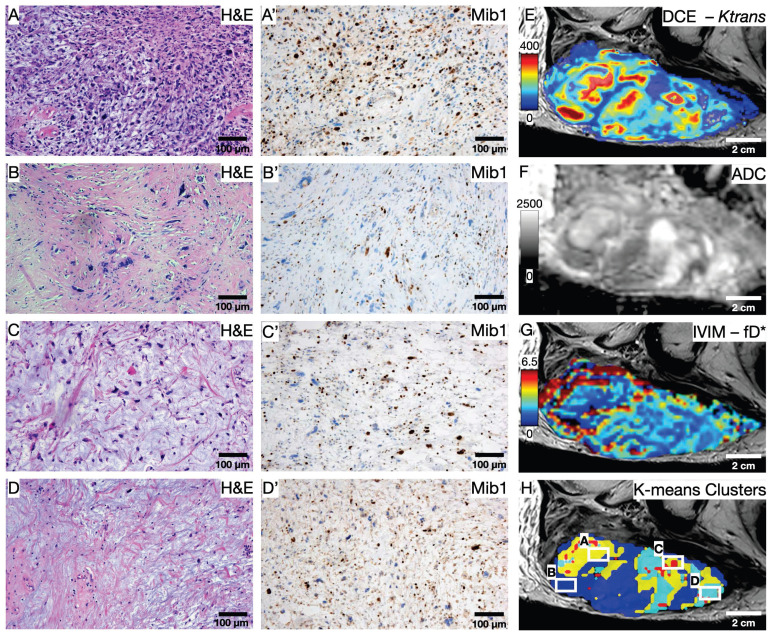
To establish a spatially exact co-registration procedure between multiparametric magnetic resonance imaging (mpMRI) and (immuno)histopathology of soft tissue sarcomas (STS) to identify imaging parameters that reflect radiation therapy response of STS. The mpMRI-Protocol included diffusion-weighted (DWI), intravoxel-incoherent motion (IVIM), and dynamic contrast-enhancing (DCE) imaging. The resection specimen was embedded in 6.5% agarose after initial fixation in formalin. To ensure identical alignment of histopathological sectioning and imaging, an MRI scan of the specimen was rigidly co-registered with the mpMRI. The deviating angulation of the specimen to the location of the tumor was determined. The agarose block was trimmed accordingly. A second MRI in a dedicated localizer with a 4 mm grid was performed, which was matched to a custom-built sectioning machine. Microtomy sections were stained with hematoxylin and eosin. Immunohistochemical staining was performed with anti-ALDH1A1 antibodies as a radioresistance and anti-MIB1 antibodies as a proliferation marker. Fusion of the digitized microtomy sections with the mpMRI was accomplished through nonrigid co-registration to the mpMRI. Co-registration accuracy was qualitatively assessed by visual assessment and quantitatively evaluated by computing target registration errors (TRE). The study sample comprised nine tumor sections from three STS patients. Visual assessment after nonrigid co-registration showed a strong morphological correlation of the histopathological specimens with MRI and mpMRI after neoadjuvant radiation therapy. Quantitative assessment of the co-registration procedure using TRE analysis of different pairs of pathology and MRI sections revealed highly accurate structural alignment, with a total median TRE of 2.25 mm (histology - MRI), 2.22 mm (histology - mpMRI), and 2.02 mm ( MRI - mpMRI). There was no significant difference between TREs of the different pairs of sections or caudal, middle, and cranial tumor parts, respectively. Our initial results show a promising approach to obtaining accurate co-registration between histopathology and MRI for STS. In a larger cohort of patients, the method established here will enable the prospective identification and validation of imaging biomarkers for radiation therapy response prediction and monitoring in STS patients via precise molecular and cellular correlation.
为了在软组织肉瘤(STS)的多参数磁共振成像(mpMRI)和(免疫)组织病理学之间建立空间精确的配准程序,以确定反映 STS 放射治疗反应的成像参数。mpMRI 方案包括扩散加权成像(DWI)、体素内不相干运动(IVIM)和动态对比增强成像(DCE)。切除标本在福尔马林初始固定后嵌入 6.5%琼脂糖中。为了确保组织病理学切片和成像的精确对齐,对标本进行刚性配准与 mpMRI。确定标本与肿瘤位置的偏离角度。相应地修剪琼脂糖块。在专用定位器中进行第二次具有 4 毫米网格的 MRI,与定制的切片机匹配。对苏木精和伊红染色的微切片进行染色。使用抗 ALDH1A1 抗体作为放射抗性和抗 MIB1 抗体作为增殖标志物进行免疫组织化学染色。通过与 mpMRI 的非刚性配准来实现数字化微切片与 mpMRI 的融合。通过视觉评估定性评估配准准确性,并通过计算目标配准误差(TRE)定量评估配准准确性。该研究样本包括来自三名 STS 患者的九个肿瘤切片。在新辅助放射治疗后,非刚性配准后的数字评估显示,组织病理学标本与 MRI 和 mpMRI 之间具有很强的形态相关性。使用不同的病理学和 MRI 切片对配准过程进行 TRE 分析的定量评估显示,结构对准高度准确,总中位数 TRE 为 2.25 毫米(组织学 - MRI)、2.22 毫米(组织学 - mpMRI)和 2.02 毫米(MRI - mpMRI)。不同切片对之间或尾、中、颅肿瘤部分的 TRE 之间没有显著差异。我们的初步结果表明,这是一种在 STS 中获得组织病理学和 MRI 之间精确配准的有前途的方法。在更大的患者队列中,这里建立的方法将能够通过精确的分子和细胞相关性,前瞻性地识别和验证用于预测和监测 STS 患者放射治疗反应的成像生物标志物。