Xiao Zilong, Wang Xinxin, Chen Xiaoxiao, Zhou Jiawei, Zhu Haitao, Zhang Jiangnan, Deng Wensheng
Department of General Surgery, First Affiliated Hospital of Nanchang University, Nanchang, China.
Laboratory of Digestive Surgery, Nanchang University, Nanchang, China.
Front Oncol. 2023 Mar 29;13:1064343. doi: 10.3389/fonc.2023.1064343. eCollection 2023.
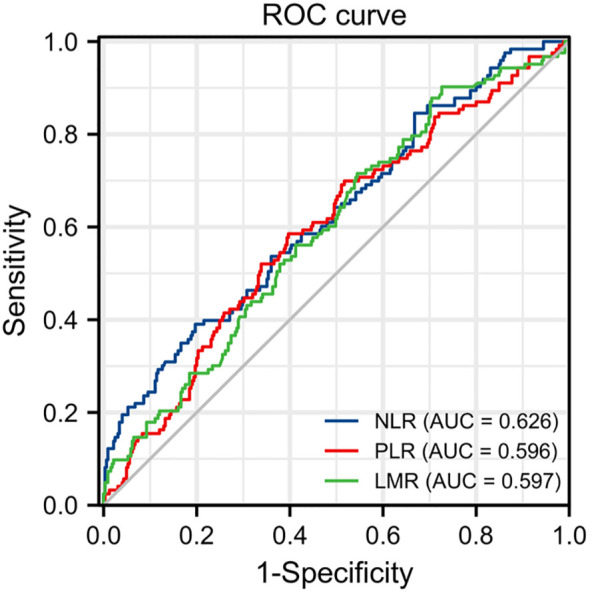
Inflammatory response markers are prognostic factors for several cancers, but their role in postoperative colorectal cancer (CRC) is unclear. The purpose was to evaluate the role of preoperative Neutrophil-to-Lymphocyte ratio (NLR), Platelet-to-Lymphocyte-ratio (PLR), and Lymphocyte-to-Monocyte ratio (LMR) in the prognosis of postoperative CRC patients.
We retrospectively reviewed 448 CRC patients who had undergone surgical resection from December 2015 to December 2017 in our hospital. The plasma NLR, PLR, LMR, CEA, and CA19-9 were collected within 2 weeks before the operation. We recorded the clinical characteristics and survival data by reviewing medical records and phone calls. We analyzed preoperative inflammatory markers and clinical features using Pearson chi-squared tests or Fisher's tests. Uni- and multivariate Cox regression analyses were performed, and overall survival (OS) was estimated with the Kaplan-Meier method.
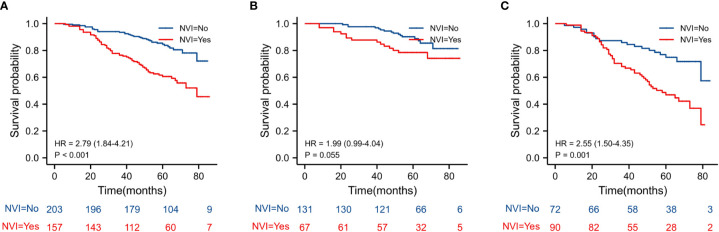
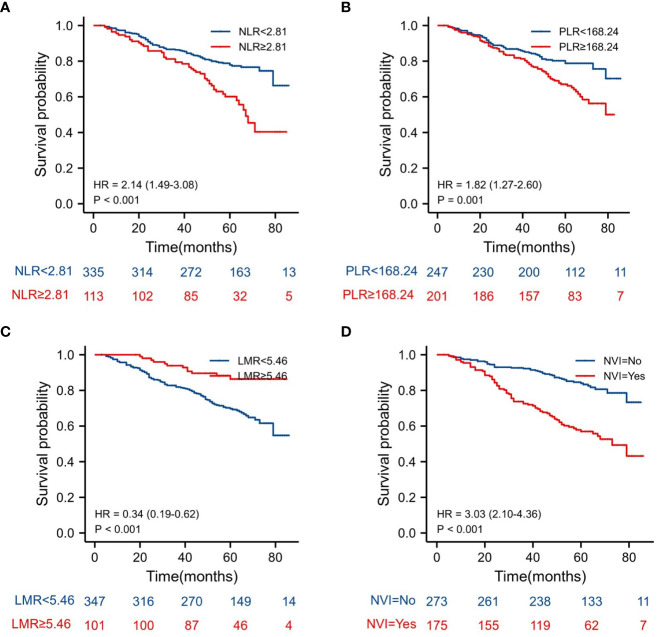
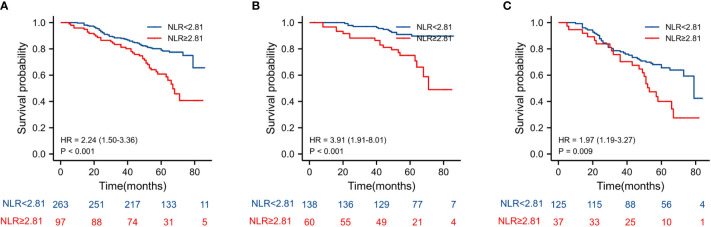
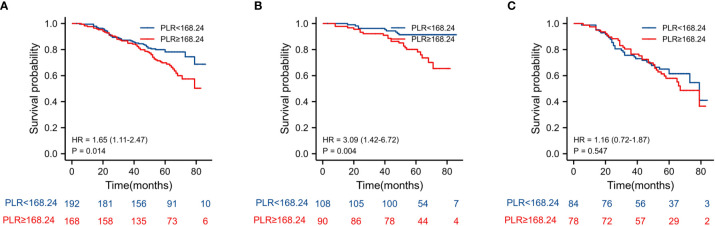
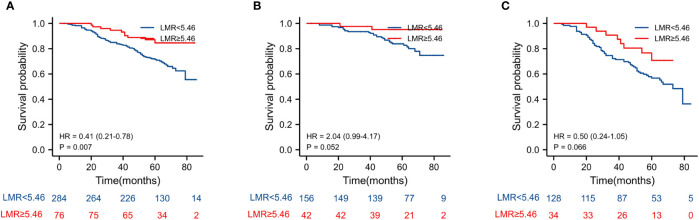
High NLR and PLR were associated with worse overall survival in postoperative CRC (HR = 2.140, 95%CI = (1.488-3.078), < 0.001; HR =1.820, 95%CI = (1.271-2.605), = 0.001). High LMR was associated with improved overall survival in postoperative CRC (HR = 0.341, 95%CI = (0.188-0.618), < 0.001). In the multivariate regression analysis, the increase of NLR resulted in an increase in the risk of death (HR = 1.678, 95%CI = (1.114-2.527), = 0.013), and for the LMR, a reduction of the risk of death (HR = 0.480, 95%CI = (0.256 - 0.902), = 0.023). Moreover, TNM stage, CA-199, CEA, nerve or vascular invasion (NVI) and adjuvant chemotherapy after surgery also were associated with worse overall survival in postoperative CRC.
Current evidence indicates that preoperative inflammatory markers NLR, LMR, and PLR are associated with overall survival in postoperative patients with colorectal cancer. NLR is an independent risk factor, and LMR is an independent protective factor in CRC patients after surgery.
炎症反应标志物是多种癌症的预后因素,但其在结直肠癌(CRC)术后的作用尚不清楚。目的是评估术前中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)和淋巴细胞与单核细胞比值(LMR)在CRC术后患者预后中的作用。
我们回顾性分析了2015年12月至2017年12月在我院接受手术切除的448例CRC患者。在手术前2周内收集血浆NLR、PLR、LMR、癌胚抗原(CEA)和糖类抗原19-9(CA19-9)。通过查阅病历和电话记录来记录临床特征和生存数据。我们使用Pearson卡方检验或Fisher检验分析术前炎症标志物和临床特征。进行单因素和多因素Cox回归分析,并采用Kaplan-Meier法估计总生存期(OS)。
高NLR和PLR与CRC术后较差的总生存期相关(风险比[HR]=2.140,95%置信区间[CI]=(1.488-3.078),P<0.001;HR=1.820,95%CI=(1.271-2.605),P=0.001)。高LMR与CRC术后总生存期改善相关(HR=0.341,95%CI=(0.188-0.618),P<0.001)。在多因素回归分析中,NLR升高导致死亡风险增加(HR=1.678,95%CI=(1.114-2.527),P=0.013),而LMR则降低死亡风险(HR=0.480,95%CI=(0.256-0.902),P=0.023)。此外,TNM分期、CA-199、CEA、神经或血管侵犯(NVI)以及术后辅助化疗也与CRC术后较差的总生存期相关。
现有证据表明,术前炎症标志物NLR、LMR和PLR与CRC术后患者的总生存期相关。NLR是一个独立的危险因素,而LMR是CRC术后患者的一个独立保护因素。