Department of Medicine, Neuchâtel Hospital Network, Neuchâtel, Switzerland.
Division of Internal Medicine, Inselspital, Bern University Hospital, Bern, Switzerland.
JAMA Intern Med. 2023 Jul 1;183(7):658-668. doi: 10.1001/jamainternmed.2023.0791.
Hospital readmissions are frequent, costly, and sometimes preventable. Although these issues have been well publicized and incentives to reduce them introduced, the best interventions for reducing readmissions remain unclear.
To evaluate the effects of a multimodal transitional care intervention targeting patients at high risk of hospital readmission on the composite outcome of 30-day unplanned readmission or death.
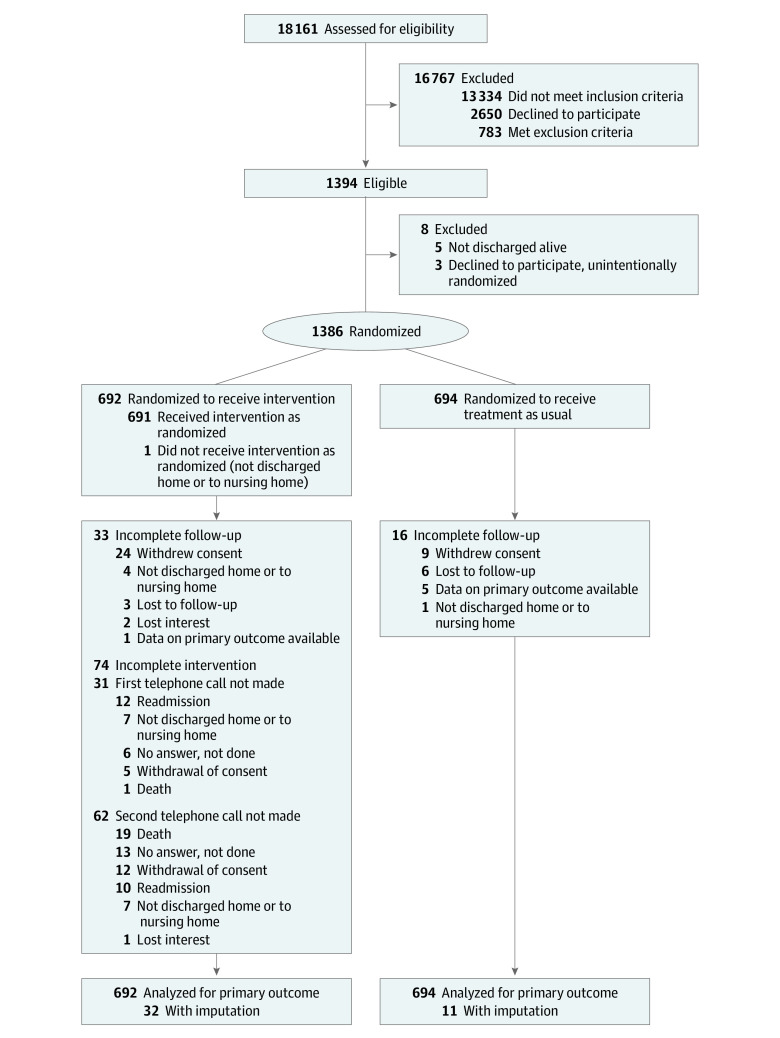
DESIGN, SETTING, AND PARTICIPANTS: A single-blinded, multicenter randomized clinical trial was conducted from April 2018 to January 2020, with a 30-day follow-up in 4 medium-to-large-sized teaching hospitals in Switzerland. Participants were consecutive patients discharged from general internal medicine wards and at higher risk of unplanned readmission based on their simplified HOSPITAL score (≥4 points). Data were analyzed between April and September 2022.
The intervention group underwent systematic medication reconciliation, a 15-minute patient education session with teach-back, a planned first follow-up visit with their primary care physician, and postdischarge follow-up telephone calls from the study team at 3 and 14 days. The control group received usual care from their hospitalist, plus a 1-page standard study information sheet.
Thirty-day postdischarge unplanned readmission or death.
A total of 1386 patients were included with a mean (SD) age of 72 (14) years; 712 (51%) were male. The composite outcome of 30-day unplanned readmission or death was 21% (95% CI, 18% to 24%) in the intervention group and 19% (95% CI, 17% to 22%) in the control group. The intention-to-treat analysis risk difference was 1.7% (95% CI, -2.5% to 5.9%; P = .44). There was no evidence of any intervention effects on time to unplanned readmission or death, postdischarge health care use, patient satisfaction with the quality of their care transition, or readmission costs.
In this randomized clinical trial, use of a standardized multimodal care transition intervention targeting higher-risk patients did not significantly decrease the risks of 30-day postdischarge unplanned readmission or death; it demonstrated the difficulties in preventing hospital readmissions, even when multimodal interventions specifically target higher-risk patients.
ClinicalTrials.gov Identifier: NCT03496896.
医院再入院频繁且费用高昂,有时甚至可以预防。尽管这些问题已经得到广泛宣传,并引入了减少再入院的激励措施,但降低再入院率的最佳干预措施仍不清楚。
评估针对高风险再入院患者的多模式过渡护理干预对 30 天内非计划性再入院或死亡的复合结局的影响。
设计、地点和参与者:这是一项单盲、多中心随机临床试验,于 2018 年 4 月至 2020 年 1 月进行,在瑞士 4 家中等至大型教学医院进行了 30 天的随访。参与者为根据简化 HOSPITAL 评分(≥4 分)确定的有较高非计划性再入院风险的普通内科病房出院患者。数据于 2022 年 4 月至 9 月进行分析。
干预组接受系统的药物重整、15 分钟的带教回授患者教育、与初级保健医生进行计划的首次随访以及出院后研究团队在第 3 天和第 14 天进行的电话随访。对照组接受其主治医生的常规治疗,外加 1 页标准研究信息表。
30 天内非计划性再入院或死亡。
共纳入 1386 例患者,平均(SD)年龄为 72(14)岁,712 例(51%)为男性。干预组 30 天内非计划性再入院或死亡的复合结局发生率为 21%(95%CI,18%24%),对照组为 19%(95%CI,17%22%)。意向治疗分析的风险差异为 1.7%(95%CI,-2.5%~5.9%;P=0.44)。没有证据表明干预对非计划性再入院或死亡时间、出院后医疗保健使用、患者对护理过渡质量的满意度或再入院费用有任何影响。
在这项随机临床试验中,使用针对高风险患者的标准化多模式护理过渡干预并没有显著降低 30 天内出院后非计划性再入院或死亡的风险;这表明,即使多模式干预专门针对高风险患者,预防医院再入院仍具有挑战性。
ClinicalTrials.gov 标识符:NCT03496896。